

CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery
- PMID: 23066360
- PMCID: PMC3459194
- DOI: 10.5664/jcsm.2140
CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery
Abstract
Background: Obstructive sleep apnea (OSA) is prevalent in the surgical population, and it has been suggested that preoperative patients should be screened and treated for OSA. However, it remains unclear whether patients diagnosed with OSA in the preoperative period adhere to prescribed CPAP therapy.
Objective: Our aim was to objectively quantify CPAP adherence, investigate predictors of poor CPAP adherence, and to establish an optimal CPAP setting in a cohort of presurgical patients diagnosed with OSA as part of the preoperative work-up.
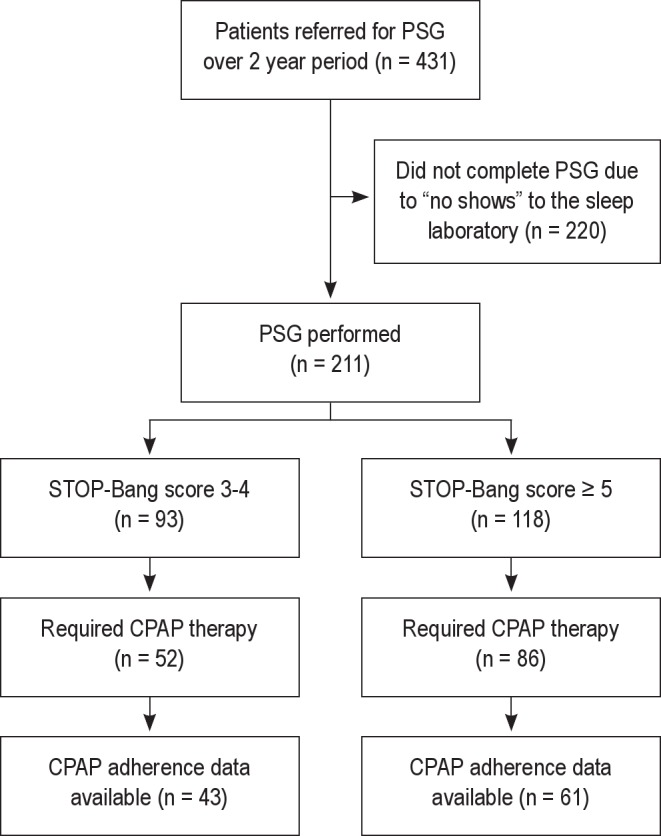
Methods: In a retrospective observational study, we collected data on all adult presurgical patients seen by the Anesthesia Perioperative Medicine Clinic (APMC) who screened positive for OSA on the STOP-Bang questionnaire and underwent an in-laboratory diagnostic polysomnogram (PSG) before surgery. CPAP was offered to patients with moderate or severe OSA. Objective CPAP adherence was recorded during the perioperative period. Factors associated with reduced CPAP adherence were delineated. Patient characteristics were compared between those with STOP-Bang scores of 3-4 and those with higher scores (STOP-Bang score ≥ 5).
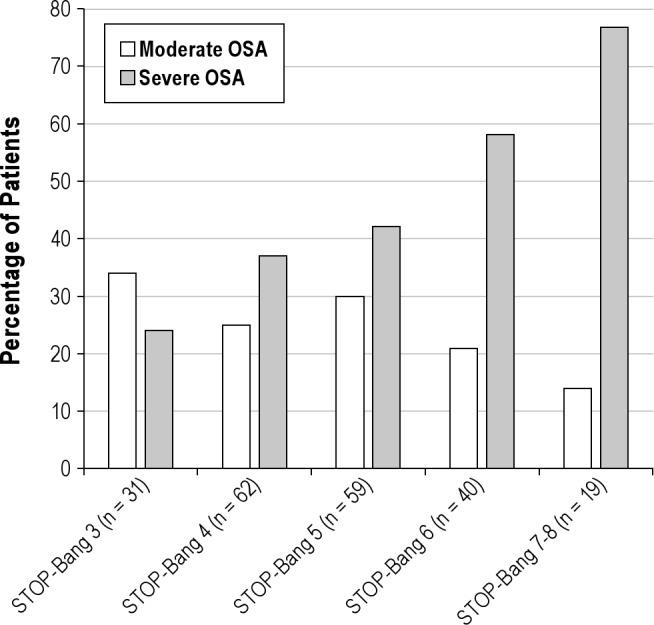
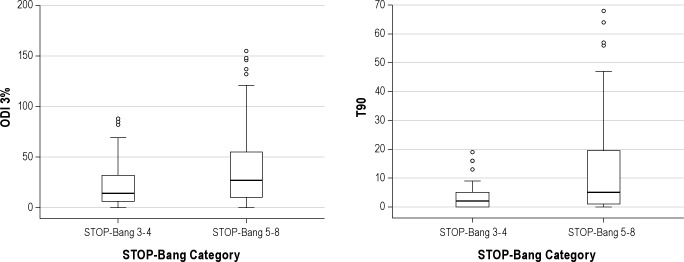
Results: During a 2-year period, 431 patients were referred and 211 patients completed a PSG. CPAP therapy was required in 65% of patients, and the optimal level was 9 ± 2 cm H(2)O. Objective CPAP adherence was available in 75% of patients who received CPAP therapy; median adherence was 2.5 h per night, without any significant difference between the STOP-Bang subgroups. African American race, male gender, and depressive symptomatology were independent predictors of reduced CPAP adherence. Severe OSA was significantly more prevalent in patients with a STOP-Bang score ≥ 5 than those whose score was 3-4 (55.1% versus 34.4%, p = 0.005). However, optimum CPAP pressure levels and adherence to therapy did not differ between the 2 STOP-Bang groups.
Conclusions: Adherence to prescribed CPAP therapy during the perioperative period was extremely low. African American race, male gender, and depressive symptoms were independently associated with reduced CPAP usage. Further research is needed to identify and overcome barriers to CPAP acceptance and adherence in the perioperative setting.
Keywords: CPAP; Obstructive sleep apnea; STOP-Bang; adherence; compliance; continuous positive airway pressure; perioperative.
Figures
Comment in
-
Is prediction of CPAP adherence in obstructive sleep apnea in the perioperative setting feasible?J Clin Sleep Med. 2013 Jul 15;9(7):731. doi: 10.5664/jcsm.2856. J Clin Sleep Med. 2013. PMID: 23853571 Free PMC article. No abstract available.
-
CPAP adherence during the perioperative period.J Clin Sleep Med. 2013 Jul 15;9(7):733-4. doi: 10.5664/jcsm.2858. J Clin Sleep Med. 2013. PMID: 23853572 Free PMC article. No abstract available.
Similar articles
-
Barriers to CPAP Use in India: An Exploratory Study.J Clin Sleep Med. 2017 Dec 15;13(12):1385-1394. doi: 10.5664/jcsm.6830. J Clin Sleep Med. 2017. PMID: 29065952 Free PMC article.
-
Adherence to Continuous Positive Airway Pressure therapy in Singaporean patients with Obstructive Sleep Apnea.Am J Otolaryngol. 2018 Sep-Oct;39(5):501-506. doi: 10.1016/j.amjoto.2018.05.012. Epub 2018 May 26. Am J Otolaryngol. 2018. PMID: 29929863
-
Predictors of long-term adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea and cardiovascular disease in the SAVE study.Sleep. 2013 Dec 1;36(12):1929-37. doi: 10.5665/sleep.3232. Sleep. 2013. PMID: 24293768 Free PMC article. Clinical Trial.
-
Perioperative Continuous Positive Airway Pressure Therapy: A Review With the Emphasis on Randomized Controlled Trials and Obstructive Sleep Apnea.Anesth Analg. 2021 May 1;132(5):1306-1313. doi: 10.1213/ANE.0000000000005480. Anesth Analg. 2021. PMID: 33857972 Review.
-
High adherence to continuous positive airway pressure (CPAP) in patients with obstructive sleep apnea (OSA) in Belgium: a narrative review.Acta Clin Belg. 2022 Jun;77(3):710-720. doi: 10.1080/17843286.2021.1943954. Epub 2021 Jul 1. Acta Clin Belg. 2022. PMID: 34197277 Review.
Cited by
-
Anaesthetic Preparation of Obese Patients: Current Status on Optimal Work-up.Curr Obes Rep. 2017 Sep;6(3):229-237. doi: 10.1007/s13679-017-0268-5. Curr Obes Rep. 2017. PMID: 28707209 Review.
-
Survey of Knowledge and Attitudes about Obstructive Sleep Apnoea Among Italian Anaesthetists.Turk J Anaesthesiol Reanim. 2017 Jun;45(3):146-152. doi: 10.5152/TJAR.2017.51423. Epub 2017 Feb 1. Turk J Anaesthesiol Reanim. 2017. PMID: 28752004 Free PMC article.
-
CPAP in the Perioperative Setting: Evidence of Support.Chest. 2016 Feb;149(2):586-597. doi: 10.1378/chest.15-1777. Epub 2016 Jan 12. Chest. 2016. PMID: 26469321 Free PMC article. Review.
-
Adherence to positive airway pressure treatment among minority populations in the US: A scoping review.Sleep Med Rev. 2018 Apr;38:56-69. doi: 10.1016/j.smrv.2017.04.002. Epub 2017 Apr 13. Sleep Med Rev. 2018. PMID: 28625480 Free PMC article.
-
Racial disparities in positive airway pressure therapy adherence among veterans with obstructive sleep apnea.J Clin Sleep Med. 2020 Aug 15;16(8):1249-1254. doi: 10.5664/jcsm.8476. J Clin Sleep Med. 2020. PMID: 32267221 Free PMC article.
References
-
- Kaw R, Pasupuleti V, Walker E, et al. Postoperative complications in patients with obstructive sleep apnea. Chest. 2012;141:436–41. - PubMed
-
- Memtsoudis S, Liu SS, Ma Y, et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg. 2011;112:113–21. - PubMed
-
- Campos-Rodriguez F, Martinez-Garcia MA, de la Cruz-Moron I, et al. Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment: a cohort study. Ann Intern Med. 2012;156:115–22. - PubMed
-
- Gami AS, Howard DE, Olson EJ, et al. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med. 2005;352:1206–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
