

Adaptive servoventilation in patients with central or complex sleep apnea related to chronic opioid use and congestive heart failure
- PMID: 23066370
- PMCID: PMC3459204
- DOI: 10.5664/jcsm.2160
Adaptive servoventilation in patients with central or complex sleep apnea related to chronic opioid use and congestive heart failure
Abstract
Study objectives: Adaptive servoventilation (ASV) is often used to treat central sleep apnea (CSA) and complex sleep apnea syndrome (CompSAS). Both CompSAS and CSA may occur in the setting of CHF and with the use of chronic opioids. We hypothesized that ASV would be less successful in treatment of CSA and CompSAS secondary to opioid use than in CHF patients.
Methods: Consecutive patients were studied between January and December 2009 who underwent ASV titration for CSA or CompSAS due to CHF (defined as EF < 45%, or > 50% with evidence for diastolic dysfunction on echocardiogram) and chronic opioid users (defined by the use of opioids > 6 months).
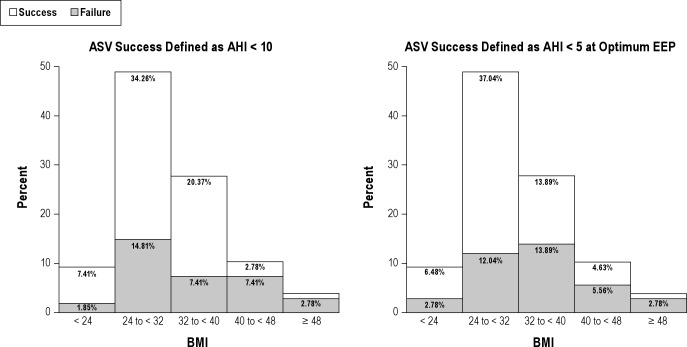
Results: Study included one hundred and eight patients with 77 males (71.3%) and 31 females (28.7%). Subjects had severe sleep apnea at baseline (AHI 45.6 ± 27.4) and inadequate control of sleep disordered breathing on CPAP (AHI 50.0 ± 32.2, CAI 36.6 ± 32). No significant differences were found between the groups in overall ASV success, defined as AHI < 10/h (p = 0.236). ASV was successful in 28 (59.6%) of those in the opioid group, compared to 43 (70.5%) of those in the CHF group. When ASV success was defined as AHI < 5/h at optimum EEP, there was again no significant difference between the groups (p-value = 0.812). Logistic regression showed unit increases in BMI, unit increases in HCO(3), and presence of CSR were each associated with decreased likelihood of ASV success.
Conclusion: We did not find a statistically significant difference in the effectiveness of ASV between CHF patients and chronic opioid users, with the overall success rate approaching 70%, as defined by an AHI < 10/h.
Commentary: A commentary on this article appears in this issue on page 577.
Keywords: Adaptive servoventilation; central sleep apnea; chronic opioid use; complex sleep apnea; congestive heart failurex.
Figures
Comment in
-
Opioid-induced sleep apnea: is it a real problem?J Clin Sleep Med. 2012 Oct 15;8(5):577-8. doi: 10.5664/jcsm.2162. J Clin Sleep Med. 2012. PMID: 23066371 Free PMC article. No abstract available.
References
-
- Practice guidelines for chronic pain management: an updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology. 2010;112:810–33. - PubMed
-
- Caravati EM, Grey T, Nangle B, et al. Increase in poisoning deaths caused by non-illicit drugs--Utah, 1991-2003. MMWR Morb Mortal Wkly Rep. 2005;54:33–6. - PubMed
-
- Moore TJ, Cohen MR, Furberg CD. Serious adverse drug events reported to the Food and Drug Administration, 1998-2005. Arch Intern Med. 2007;167:1752–9. - PubMed
-
- Pepperell JC, Maskell NA, Jones DR, et al. A randomized controlled trial of adaptive ventilation for Cheyne-Stokes breathing in heart failure. Am J Respir Crit Care Med. 2003;168:1109–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
