

The relationship between serum sodium and intracranial pressure when using hypertonic saline to target mild hypernatremia in patients with head trauma
- PMID: 23068293
- PMCID: PMC3682295
- DOI: 10.1186/cc11678
The relationship between serum sodium and intracranial pressure when using hypertonic saline to target mild hypernatremia in patients with head trauma
Abstract
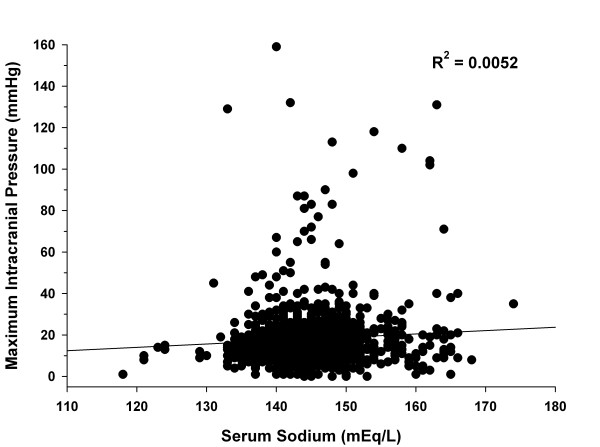
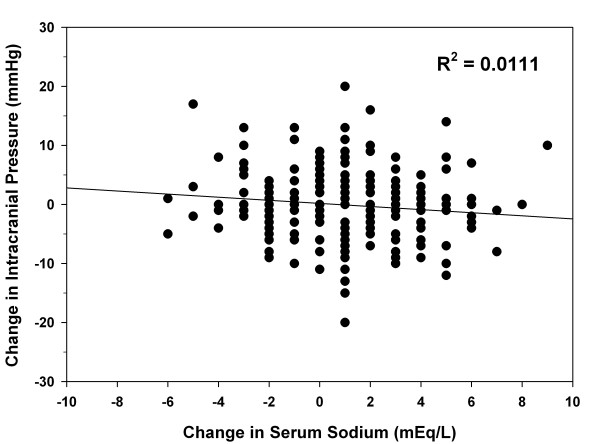
Introduction: Limited data suggest mild hypernatremia may be related to lower intracranial pressure (ICP) in patients with traumatic brain injury (TBI). The practice at the study center has been to use hypertonic saline (HTS) to generate a targeted serum sodium of 145 to 155 mEq/l in patients with TBI. The purpose of this study was to determine the relationship between serum sodium values and ICP, and to evaluate the acute effect of HTS on ICP.
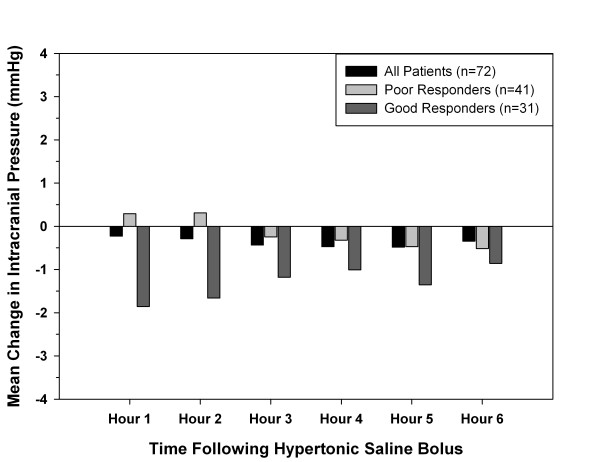
Methods: A retrospective review of patients who were admitted to the trauma ICU for TBI, had an ICP monitor placed, and received at least one dose of HTS between January 2006 and March 2011 was performed. Data were collected for up to 120 hours after ICP monitor placement. The primary outcome was the relationship between serum sodium and maximum ICP. Secondary outcomes were the relationship between serum sodium and the mean number of daily interventions for ICP control, and the acute effect of HTS on ICP during the 6 hours after each dose. Linear regression was used to analyze the primary outcome. Analysis of variance on ranks and repeated measures analysis of variance were used to evaluate the number of interventions and the acute effect of HTS on ICP, respectively.
Results: Eighty-one patients were enrolled with mean ± standard deviation age of 36 ± 15 years and median Glasgow Coma Scale score of 7 (interquartile range, 4 to 7). A total of 1,230 serum sodium values (range, 118 to 174 mEq/l) and 7,483 ICP values (range, 0 to 159 mmHg) were collected. There was no correlation between serum sodium and maximum ICP (R(2) = 0.0052). The overall mean ± standard deviation number of interventions for elevated ICP per day was 4.2 ± 2.9, 2.9 ± 2.0, and 2.6 ± 2.3 for patients with a mean serum sodium of < 145, 145 to 155, and > 155 mEq/l, respectively (P < 0.001). Regarding the acute effect of HTS on ICP, there was no statistical difference in mean ICP compared with baseline during hours 1 through 6 following HTS doses (baseline, 13.7 ± 8.4 mmHg; hour 1, 13.6 ± 8.3 mmHg; hour 2, 13.5 ± 8.8 mmHg; hour 3, 13.3 ± 8.7 mmHg; hour 4, 13.4 ± 8.7 mmHg; hour 5, 13.4 ± 8.3 mmHg; hour 6, 13.5 ± 8.3 mmHg; P = 0.84).
Conclusions: Serum sodium concentrations did not correlate with ICP values. These results warrant further evaluation and possible reassessment of sodium goals for ICP management in patients with TBI.
Figures
Comment in
-
Hypernatremia and intracranial pressure: more questions than answers.Crit Care. 2013 Jan 7;17(1):401. doi: 10.1186/cc11888. Crit Care. 2013. PMID: 23294598 Free PMC article.
-
Authors' response.Crit Care. 2013;17(1):401. Crit Care. 2013. PMID: 25215361 No abstract available.
References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;16:375–378. - PubMed
-
- Brain Trauma Foundation, American Association of Neurological Surgeons Joint Section on Neurotrauma and Critical Care. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2007;16(Suppl 1):S1–S106. - PubMed
-
- Kofke WA. Mannitol: potential for rebound intracranial hypertension? J Neurosurg Anesthesiol. 1993;16:1–3. - PubMed
-
- Vialet R, Albanèse J, Thomachot L, Antonini F, Bourgouin A, Alliez B, Martin C. Isovolume hypertonic solutes (sodium chloride or mannitol) in the treatment of refractory posttraumatic intracranial hypertension: 2 mL/kg 7.5% saline is more effective than 2 mL/kg 20% mannitol. Crit Care Med. 2003;16:1683–1687. doi: 10.1097/01.CCM.0000063268.91710.DF. - DOI - PubMed
-
- Ware ML, Nemani VM, Meeker M, Lee C, Morabito DJ, Manley GT. Effects of 23.4% sodium chloride solution in reducing intracranial pressure in patients with traumatic brain injury: a preliminary study. Neurosurgery. 2005;16:727–736. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
