

Treatment options for central retinal artery occlusion
- PMID: 23070637
- PMCID: PMC3553407
- DOI: 10.1007/s11940-012-0202-9
Treatment options for central retinal artery occlusion
Abstract
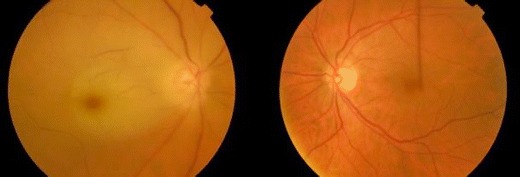
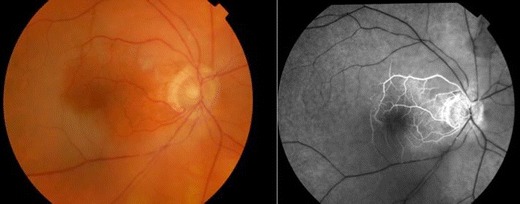
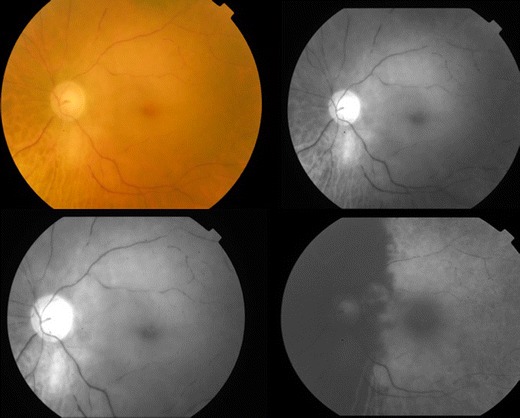
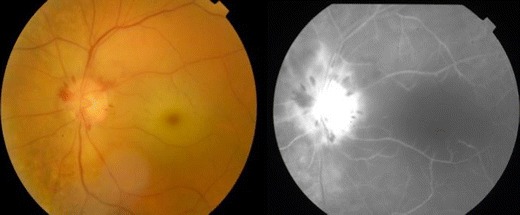
Central retinal artery occlusion (CRAO) is an ocular emergency and is the ocular analogue of cerebral stroke. It results in profound, usually monocular vision loss, and is associated with significant functional morbidity. The risk factors for CRAO are the same atherosclerotic risk factors as for stroke and heart disease. As such, individuals with CRAO may be at risk of ischemic end organ damage such as a cerebral stroke. Therefore, the management of CRAO is not only to restore vision, but at the same time to manage risk factors that may lead to other vascular conditions. There are a number of therapies that has been used in the treatment of CRAO in the past. These include carbogen inhalation, acetazolamide infusion, ocular massage and paracentesis, as well as various vasodilators such as intravenous glyceryl trinitrate. None of these "standard agents" have been shown to alter the natural history of disease definitively. There has been recent interest shown in the use of thrombolytic therapy, delivered either intravenously or intra-arterially by direct catheterisation of the ophthalmic artery. Whilst a number of observational series have shown that the recovery of vision can be quite dramatic, two recent randomised controlled trials have not demonstrated efficacy. On the contrary, intra-arterial delivery of thrombolytic may result in an increased risk of intracranial and systemic haemorrhage, while the intravenous use of tissue plasminogen activator (tPA) was not shown to be efficacious within 24 h of symptom onset. Nevertheless, both of these studies have shown one thing in common, and that is for treatment to be effective in CRAO, it must be deployed within a short time window, probably within 6 h of symptom onset. Therefore, while CRAO is a disease that does not have a treatment, nevertheless it needs to follow the same principles of treatment as any other vascular end organ ischaemic disease. That is, to attempt to reperfuse ischemic tissue as quickly as possible and to institute secondary prevention early.
Figures
References
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
-
- Graefes AV. Ueber Embolie der Arteria centralis retinae als Ursache plotzlicher Erblindung. Arch Ophthalmol;5:136–157
-
- Lorentzen S. Incidence of cilioretinal arteries. Acta Ophthalmol. 1970;48:518–524. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
