

Prognosis of patients with hepatocellular carcinoma. Validation and ranking of established staging-systems in a large western HCC-cohort
- PMID: 23071507
- PMCID: PMC3465308
- DOI: 10.1371/journal.pone.0045066
Prognosis of patients with hepatocellular carcinoma. Validation and ranking of established staging-systems in a large western HCC-cohort
Abstract
Background: HCC is diagnosed in approximately half a million people per year, worldwide. Staging is a more complex issue than in most other cancer entities and, mainly due to unique geographic characteristics of the disease, no universally accepted staging system exists to date. Focusing on survival rates we analyzed demographic, etiological, clinical, laboratory and tumor characteristics of HCC-patients in our institution and applied the common staging systems. Furthermore we aimed at identifying the most suitable of the current staging systems for predicting survival.
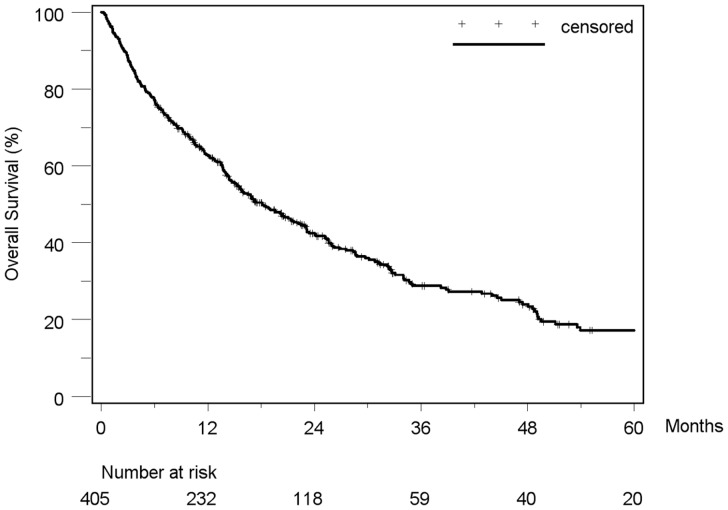
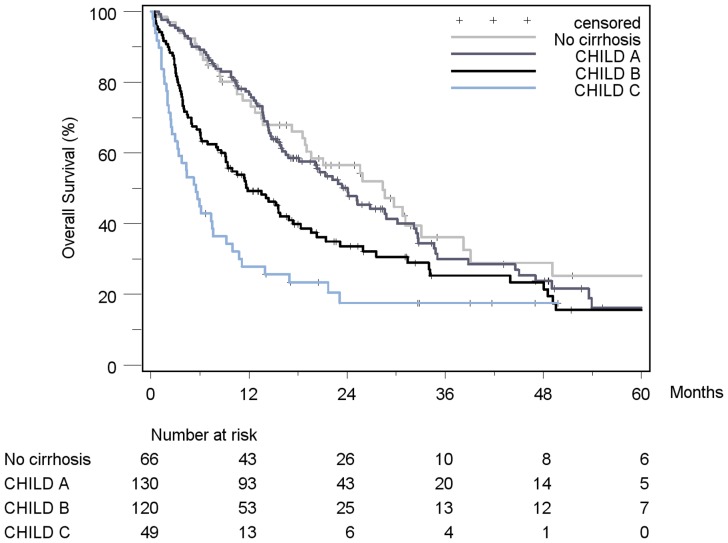
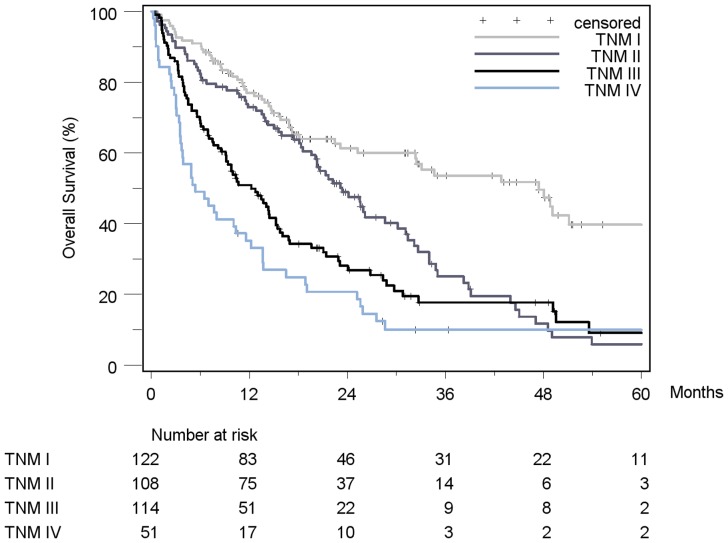
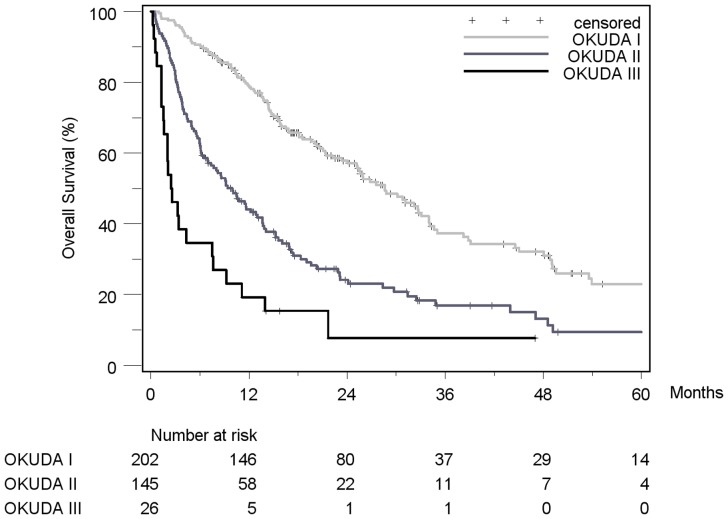
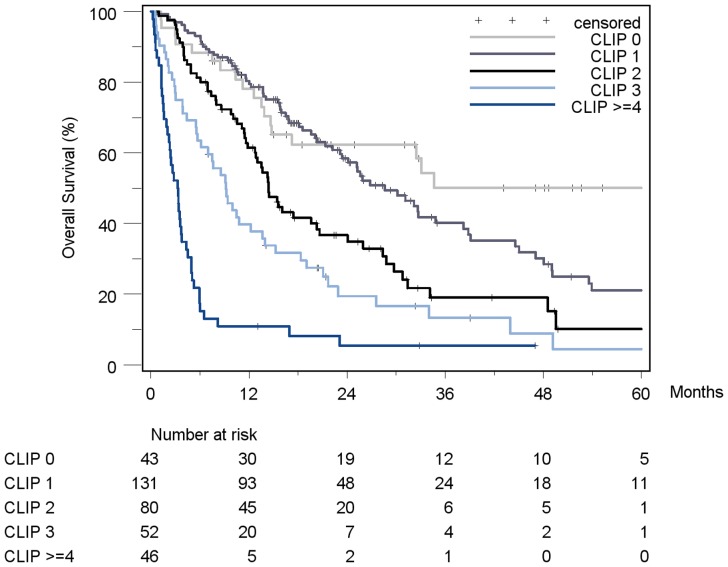
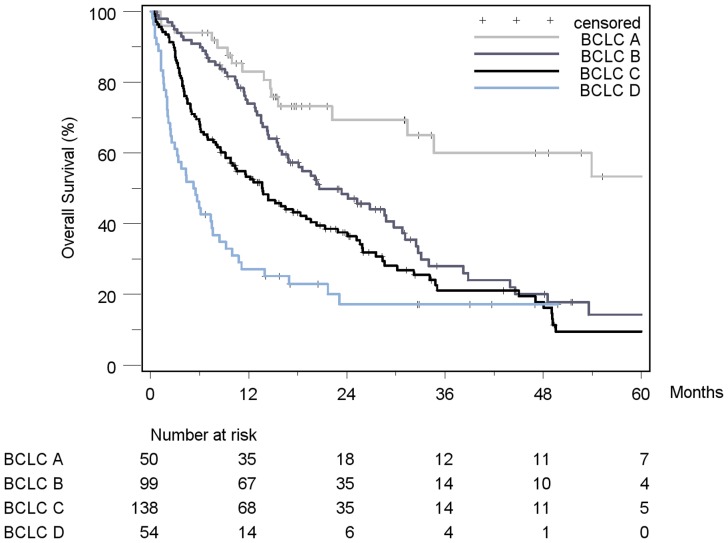
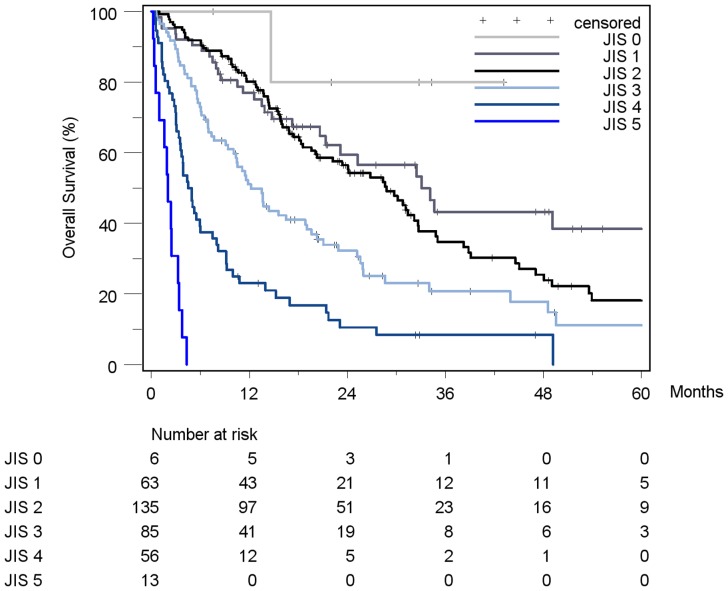
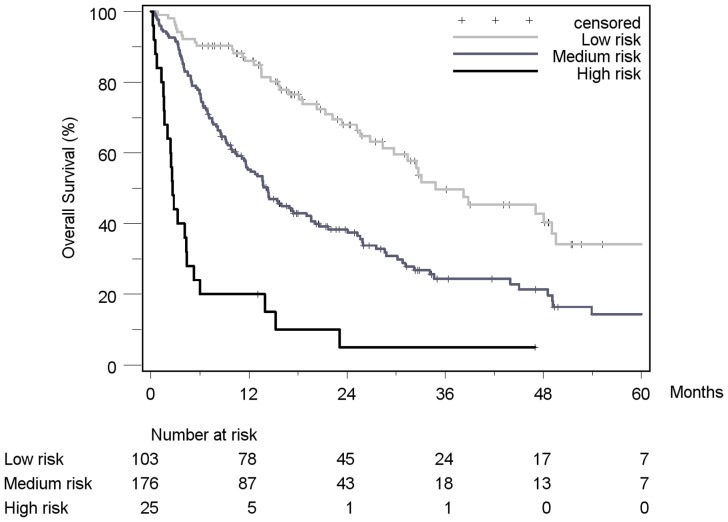
Methodology/principal findings: Overall, 405 patients with HCC were identified from an electronic medical record database. The following seven staging systems were applied and ranked according to their ability to predict survival by using the Akaike information criterion (AIC) and the concordance-index (c-index): BCLC, CLIP, GETCH, JIS, Okuda, TNM and Child-Pugh. Separately, every single variable of each staging system was tested for prognostic meaning in uni- and multivariate analysis. Alcoholic cirrhosis (44.4%) was the leading etiological factor followed by viral hepatitis C (18.8%). Median survival was 18.1 months (95%-CI: 15.2-22.2). Ascites, bilirubin, alkaline phosphatase, AFP, number of tumor nodes and the BCLC tumor extension remained independent prognostic factors in multivariate analysis. Overall, all of the tested staging systems showed a reasonable discriminatory ability. CLIP (closely followed by JIS) was the top-ranked score in terms of prognostic capability with the best values of the AIC and c-index (AIC 2286, c-index 0.71), surpassing other established staging systems like BCLC (AIC 2343, c-index 0.66). The unidimensional scores TNM (AIC 2342, c-index 0.64) and Child-Pugh (AIC 2369, c-index 0.63) performed in an inferior fashion.
Conclusions/significance: Compared with six other staging systems, the CLIP-score was identified as the most suitable staging system for predicting prognosis in a large German cohort of predominantly non-surgical HCC-patients.
Conflict of interest statement
Figures
Similar articles
-
Prognosis of unresectable hepatocellular carcinoma: comparison of seven staging systems (TNM, Okuda, BCLC, CLIP, CUPI, JIS, CIS) in a Chinese cohort.PLoS One. 2014 Mar 7;9(3):e88182. doi: 10.1371/journal.pone.0088182. eCollection 2014. PLoS One. 2014. PMID: 24609114 Free PMC article.
-
Validation and ranking of seven staging systems of hepatocellular carcinoma.Oncol Lett. 2017 Jul;14(1):705-714. doi: 10.3892/ol.2017.6222. Epub 2017 May 22. Oncol Lett. 2017. PMID: 28693224 Free PMC article.
-
Evaluation of predictive value of CLIP, Okuda, TNM and JIS staging systems for hepatocellular carcinoma patients undergoing surgery.J Gastroenterol Hepatol. 2005 May;20(5):765-71. doi: 10.1111/j.1440-1746.2005.03746.x. J Gastroenterol Hepatol. 2005. PMID: 15853992
-
Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score).J Gastroenterol. 2003;38(3):207-15. doi: 10.1007/s005350300038. J Gastroenterol. 2003. PMID: 12673442 Review.
-
Advances in post-operative prognostic models for hepatocellular carcinoma.J Zhejiang Univ Sci B. 2023 Mar 15;24(3):191-206. doi: 10.1631/jzus.B2200067. J Zhejiang Univ Sci B. 2023. PMID: 36915996 Free PMC article. Review.
Cited by
-
Biodistribution Profile of Magnetic Nanoparticles in Cirrhosis-Associated Hepatocarcinogenesis in Rats by AC Biosusceptometry.Pharmaceutics. 2022 Sep 8;14(9):1907. doi: 10.3390/pharmaceutics14091907. Pharmaceutics. 2022. PMID: 36145654 Free PMC article.
-
Development and validation of a risk score for predicting mortality after resection of primary hepatocellular carcinoma.Aging (Albany NY). 2020 Jun 21;12(12):11878-11892. doi: 10.18632/aging.103360. Epub 2020 Jun 21. Aging (Albany NY). 2020. PMID: 32568098 Free PMC article.
-
Comparing staging systems for predicting prognosis and survival in patients with hepatocellular carcinoma in Egypt.PLoS One. 2014 Mar 6;9(3):e90929. doi: 10.1371/journal.pone.0090929. eCollection 2014. PLoS One. 2014. PMID: 24603710 Free PMC article.
-
Phase I study of nintedanib in Japanese patients with advanced hepatocellular carcinoma and liver impairment.Cancer Sci. 2016 Dec;107(12):1791-1799. doi: 10.1111/cas.13077. Epub 2016 Dec 12. Cancer Sci. 2016. PMID: 27627050 Free PMC article. Clinical Trial.
-
Overview of Prognostic Systems for Hepatocellular Carcinoma and ITA.LI.CA External Validation of MESH and CNLC Classifications.Cancers (Basel). 2021 Apr 2;13(7):1673. doi: 10.3390/cancers13071673. Cancers (Basel). 2021. PMID: 33918125 Free PMC article. Review.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, et al. (2011) Global cancer statistics. CA Cancer J Clin 6: 69–90. - PubMed
-
- Poon D, Anderson BO, Chen LT, Tanaka K, Lau WY, et al. (2009) Management of hepatocellular carcinoma in Asia: consensus statement from the Asian Oncology Summit 2009. Lancet Oncol 10: 1111–8. - PubMed
-
- Sherman M (2005) Hepatocellular Carcinoma: Epidemiology, Risk Factors, and Screening. Semin Liver Dis 25: 143–154. - PubMed
-
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, et al. (2007) Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 18: 581–92. - PubMed
-
- Lei HJ, Chau GY, Lui WY (2006) Prognostic value and clinical relevance of the 6th Edition 2002 American Joint Committee on Cancer staging system in patients with resectable hepatocellular carcinoma. J Am Coll Surg 203: 426–435. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
