

Plasma uric acid levels correlate with inflammation and disease severity in Malian children with Plasmodium falciparum malaria
- PMID: 23071567
- PMCID: PMC3465329
- DOI: 10.1371/journal.pone.0046424
Plasma uric acid levels correlate with inflammation and disease severity in Malian children with Plasmodium falciparum malaria
Abstract
Background: Plasmodium falciparum elicits host inflammatory responses that cause the symptoms and severe manifestations of malaria. One proposed mechanism involves formation of immunostimulatory uric acid (UA) precipitates, which are released from sequestered schizonts into microvessels. Another involves hypoxanthine and xanthine, which accumulate in parasitized red blood cells (RBCs) and may be converted by plasma xanthine oxidase to UA at schizont rupture. These two forms of 'parasite-derived' UA stimulate immune cells to produce inflammatory cytokines in vitro.
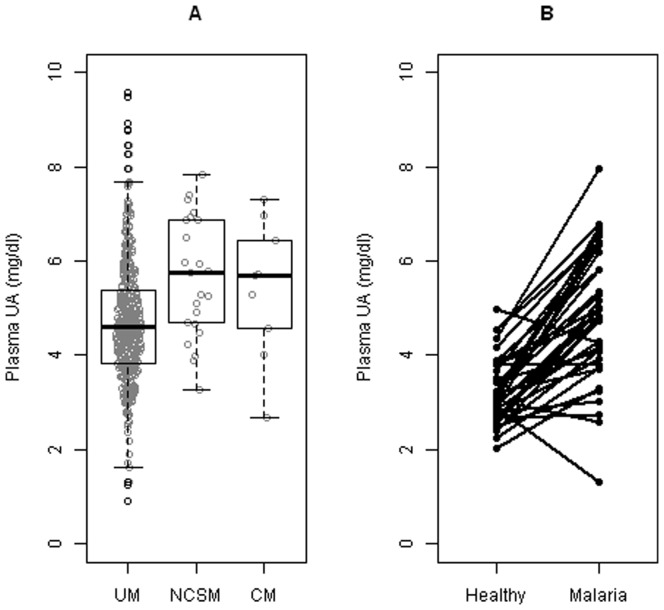
Methods and findings: We measured plasma levels of soluble UA and inflammatory cytokines and chemokines (IL-6, IL-10, sTNFRII, MCP-1, IL-8, TNFα, IP-10, IFNγ, GM-CSF, IL-1β) in 470 Malian children presenting with uncomplicated malaria (UM), non-cerebral severe malaria (NCSM) or cerebral malaria (CM). UA levels were elevated in children with NCSM (median 5.74 mg/dl, 1.21-fold increase, 95% CI 1.09-1.35, n = 23, p = 0.0007) and CM (median 5.69 mg/dl, 1.19-fold increase, 95% CI 0.97-1.41, n = 9, p = 0.0890) compared to those with UM (median 4.60 mg/dl, n = 438). In children with UM, parasite density and plasma creatinine levels correlated with UA levels. These UA levels correlated with the levels of seven cytokines [IL-6 (r = 0.259, p<0.00001), IL-10 (r = 0.242, p<0.00001), sTNFRII (r = 0.221, p<0.00001), MCP-1 (r = 0.220, p<0.00001), IL-8 (r = 0.147, p = 0.002), TNFα (r = 0.132, p = 0.006) and IP-10 (r = 0.120, p = 0.012)]. In 39 children, UA levels were 1.49-fold (95% CI 1.34-1.65; p<0.0001) higher during their malaria episode [geometric mean titer (GMT) 4.67 mg/dl] than when they were previously healthy and aparasitemic (GMT 3.14 mg/dl).
Conclusions: Elevated UA levels may contribute to the pathogenesis of P. falciparum malaria by activating immune cells to produce inflammatory cytokines. While this study cannot identify the cause of elevated UA levels, their association with parasite density and creatinine levels suggest that parasite-derived UA and renal function may be involved. Defining pathogenic roles for parasite-derived UA precipitates, which we have not directly studied here, requires further investigation.
Trial registration: ClinicalTrials.gov NCT00669084.
Conflict of interest statement
Figures
References
-
- World Health Organization. World Malaria Report 2012.
-
- Murray CJ, Rosenfeld LC, Lim SS, Andrews KG, Foreman KJ, et al. (2012) Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet 379: 413–431. - PubMed
-
- Van Den Steen PE, Deroost K, Geurts N, Heremans H, Van Damme J, et al. (2011) Malaria: host-pathogen interactions, immunopathological complications and therapy. Verh K Acad Geneeskd Belg 73: 123–151. - PubMed
-
- Higgins SJ, Kain KC, Liles WC (2011) Immunopathogenesis of falciparum malaria: implications for adjunctive therapy in the management of severe and cerebral malaria. Expert Rev Anti Infect Ther 9: 803–819. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
