

The effect of complete integration of HIV and TB services on time to initiation of antiretroviral therapy: a before-after study
- PMID: 23071690
- PMCID: PMC3465310
- DOI: 10.1371/journal.pone.0046988
The effect of complete integration of HIV and TB services on time to initiation of antiretroviral therapy: a before-after study
Abstract
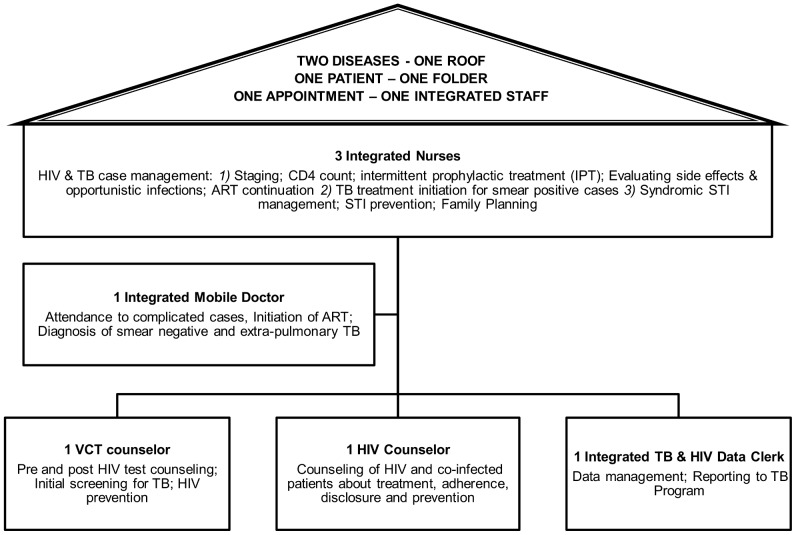
Background: Studies have shown that early ART initiation in TB/HIV co-infected patients lowers mortality. One way to implement earlier ART commencement could be through integration of TB and HIV services, a more efficient model of care than separate, vertical programs. We present a model of full TB/HIV integration and estimate its effect on time to initiation of ART.
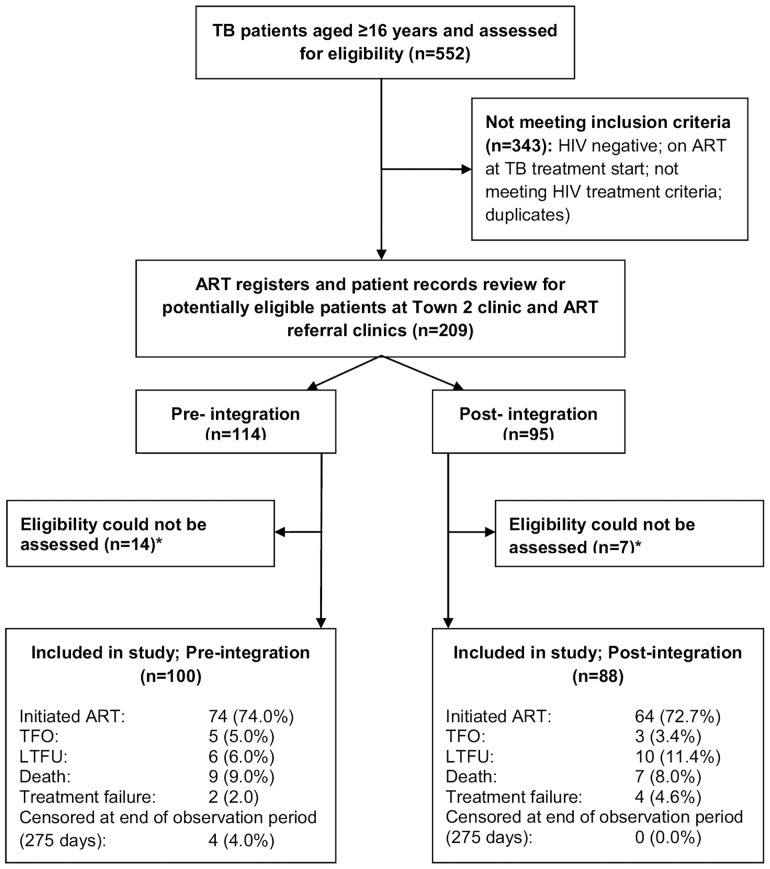
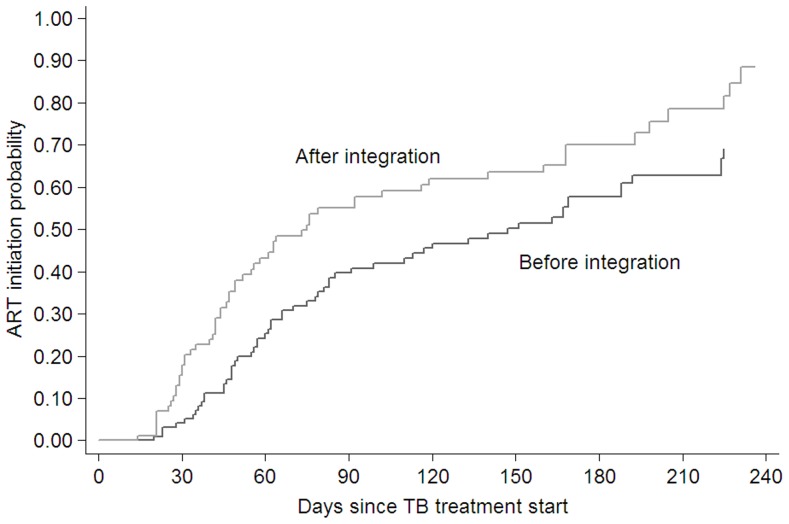
Methodology/principal findings: We retrospectively reviewed TB registers and clinical notes of 209 TB/HIV co-infected adults with a CD4 count <250 cells/µl and registered for TB treatment at one primary care clinic in a South African township between June 2008 and May 2009. Using Kaplan-Meier and Cox proportional hazard analysis, we compared time between initiation of TB treatment and ART for the periods before and after full, "one-stop shop" integration of TB and HIV services (in December 2009). Potential confounders were determined a priori through directed acyclic graphs. Robustness of assumptions was investigated by sensitivity analyses. The analysis included 188 patients (100 pre- and 88 post-integration), yielding 56 person-years of observation. Baseline characteristics of the two groups were similar. Median time to ART initiation decreased from 147 days (95% confidence interval [CI] 85-188) before integration of services to 75 days (95% CI 52-119) post-integration. In adjusted analyses, patients attending the clinic post-integration were 1.60 times (95% CI 1.11-2.29) more likely to have started ART relative to the pre-integration period. Sensitivity analyses supported these findings.
Conclusions/significance: Full TB/HIV care integration is feasible and led to a 60% increased chance of co-infected patients starting ART, while reducing time to ART initiation by an average of 72 days. Although these estimates should be confirmed through larger studies, they suggest that scale-up of full TB/HIV service integration in high TB/HIV prevalence settings may shorten time to ART initiation, which might reduce excess mortality and morbidity.
Conflict of interest statement
Figures
References
-
- UNAIDS (2010) Global report: UNAIDS report on the global AIDS epidemic 2010. UNAIDS.
-
- World Health Organisation (2010) Global tuberculosis control: WHO report 2010. Geneva: WHO.
-
- Naidoo S, Taylor M, Jinabhai C (2007) Critical risk factors driving the tuberculosis epidemic in KwaZulu-Natal, South Africa. The Southern African Journal of Epidemiology and Infection 22: 45–49.
-
- Wells CD, Cegielski JP, Nelson LJ, Laserson KF, Holtz TH, et al. (2007) HIV Infection and Multidrug-Resistant Tuberculosis–The Perfect Storm. The Journal of Infectious Diseases 196: S86–S107. - PubMed
-
- Andrews JR, Shah NS, Gandhi N, Moll T, Friedland G (2007) Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: Implications for the HIV Epidemic and Antiretroviral Therapy Rollout in South Africa. The Journal of Infectious Diseases 196: S482–S490. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
