

Anomalous systemic artery to a normal lung: a rare cause of hemoptysis in adults
- PMID: 23071887
- PMCID: PMC3464741
- DOI: 10.5001/omj.2012.79
Anomalous systemic artery to a normal lung: a rare cause of hemoptysis in adults
Abstract
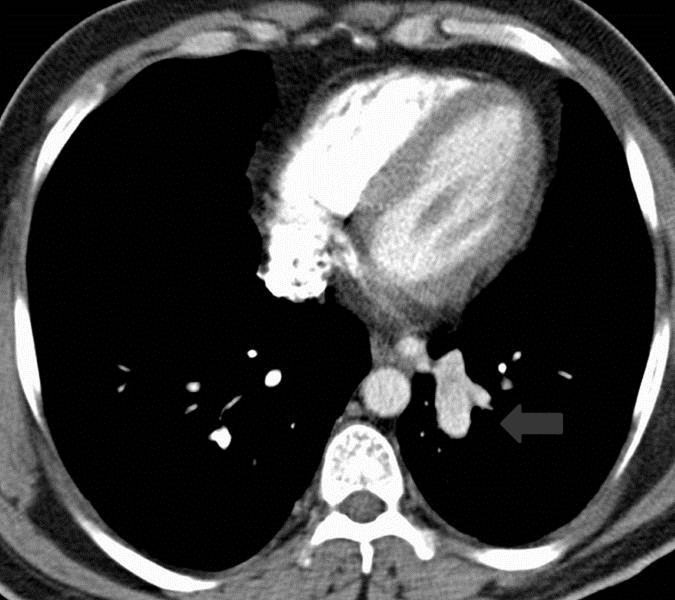
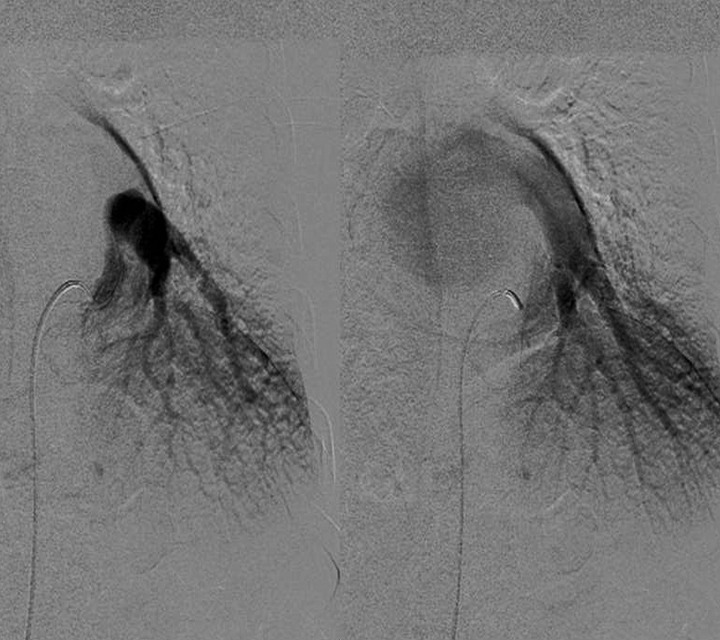
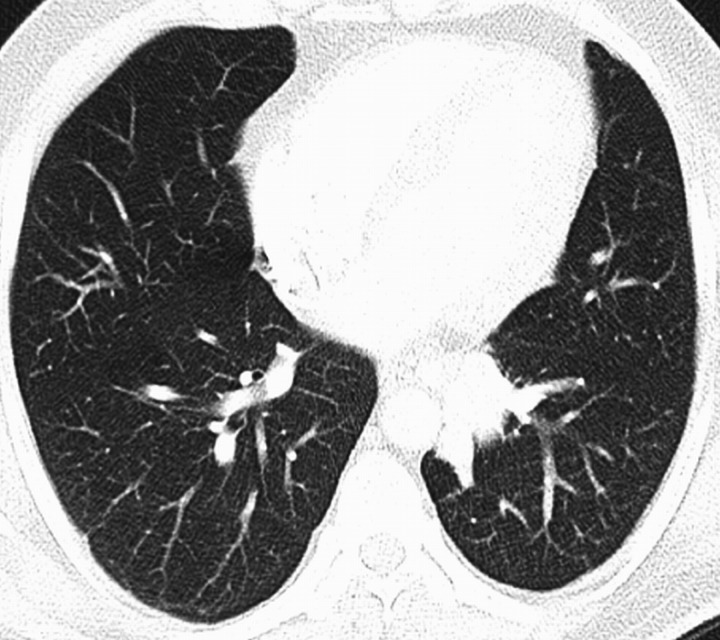
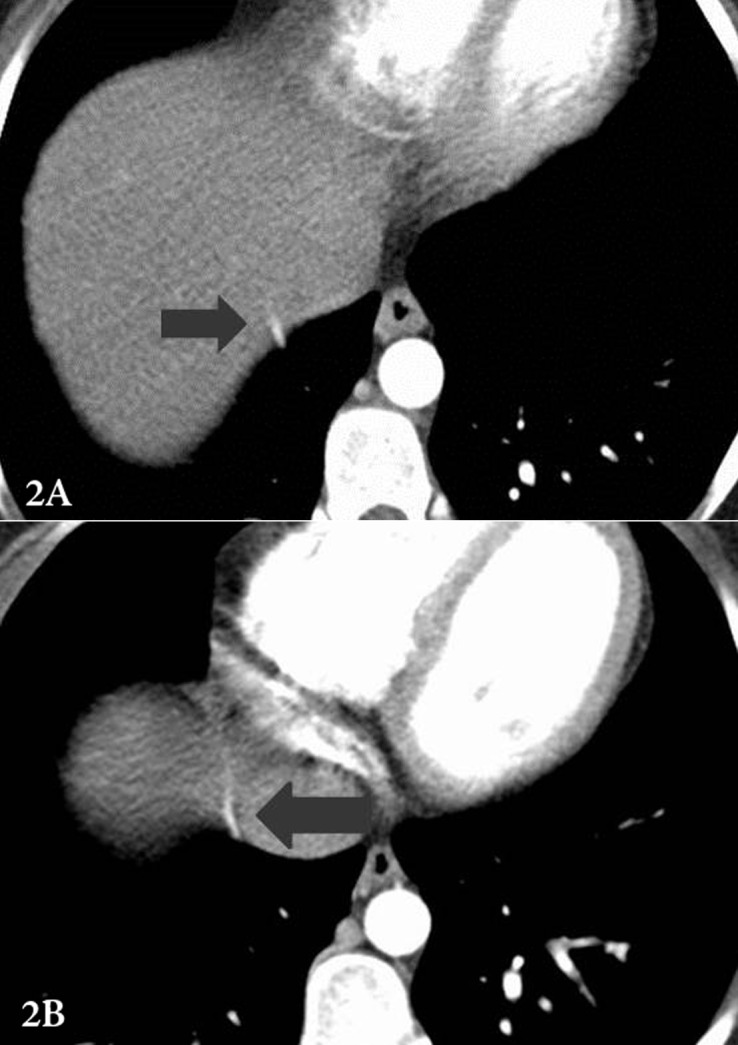
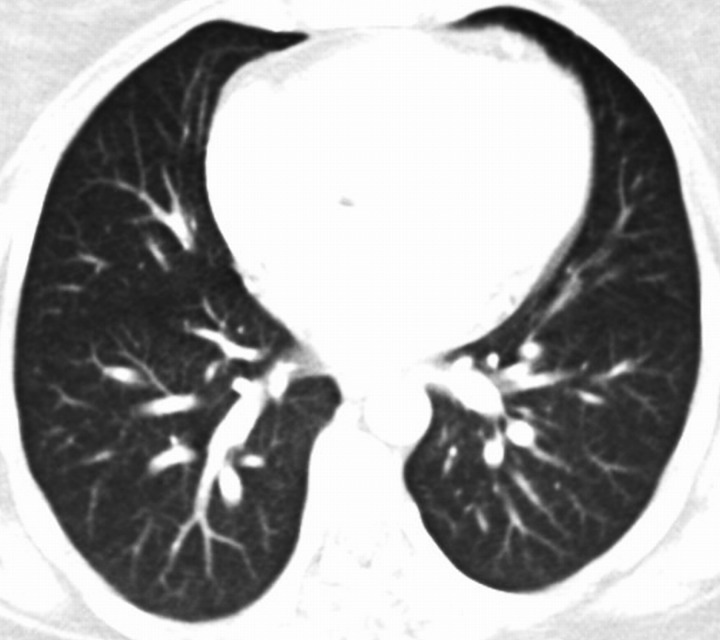
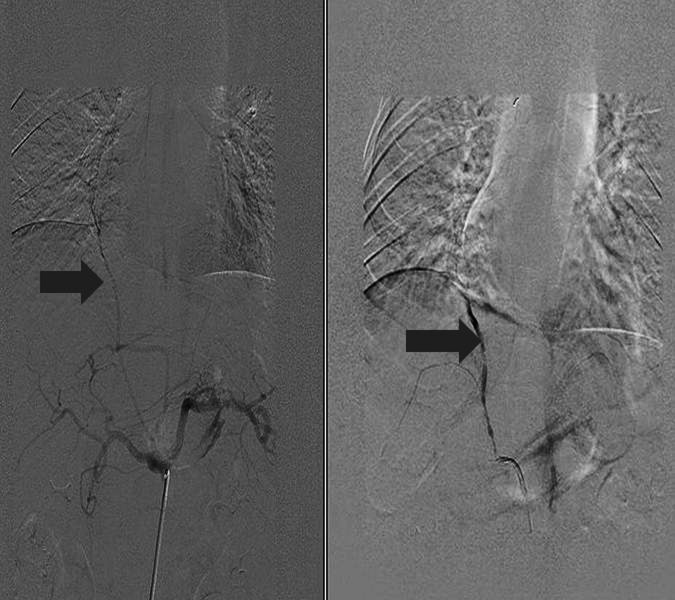
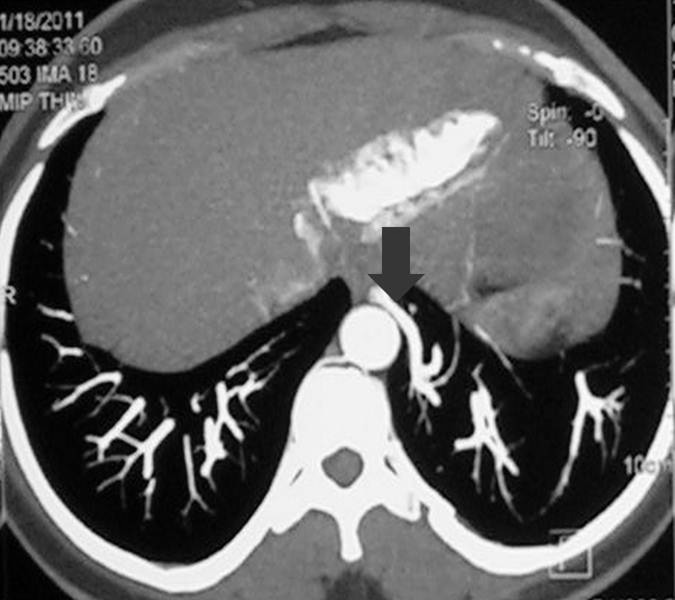
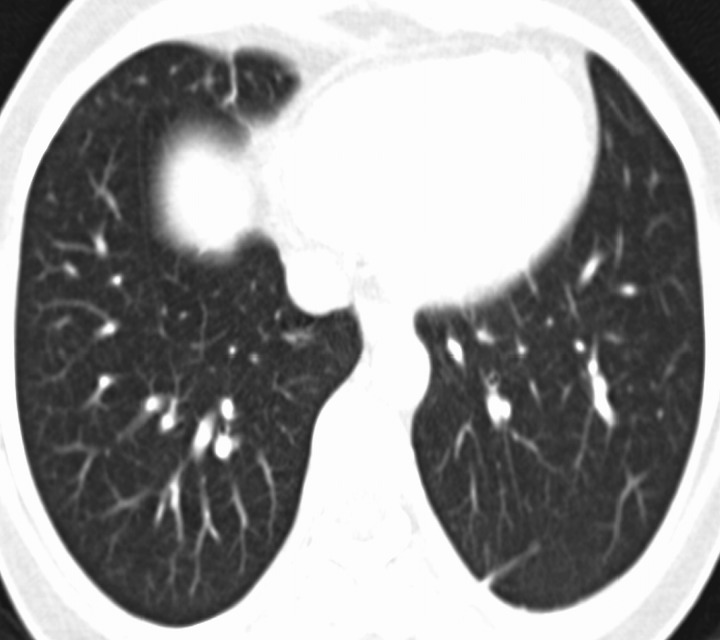
Bronchopulmonary sequestration represents a spectrum of abnormalities. One of these abnormalities is an aberrant systemic arterial supply to a normal lung with no bronchial sequestration. These lesions were originally classified by Pryce as type 1. Most of these patients are asymptomatic but with time, many patients develop localized pulmonary hypertension, hemoptysis, and eventually high output cardiac failure. Multidetector computed tomography (MDCT) plays an important role in the diagnosis and planning of definitive treatment by identifying the origin and course of the aberrant artery. Definitive treatment can be surgical (lobectomy or segmentectomy) or endovascular.
Keywords: Hemoptysis; Pryce type 1; Sequestration.
Figures


References
-
- Ellis K. Fleischner lecture. Developmental abnormalities in the systemic blood supply to the lungs. AJR Am J Roentgenol 1991. Apr;156(4):669-679 - PubMed
Publication types
LinkOut - more resources
Full Text Sources