

Near-universal prevalence of Pneumocystis and associated increase in mucus in the lungs of infants with sudden unexpected death
- PMID: 23074306
- PMCID: PMC3526255
- DOI: 10.1093/cid/cis870
Near-universal prevalence of Pneumocystis and associated increase in mucus in the lungs of infants with sudden unexpected death
Abstract
Background: Pneumocystis without obvious accompanying pathology is occasionally reported in autopsied infant lungs. Its prevalence and significance are unknown. Interestingly, this mild infection induces a strong activation of mucus secretion-related genes in young immunocompetent rodents that has not been explored in infants. Excess mucus is induced by multiple airway offenders through nonspecific pathways and would explain a cofactor role of Pneumocystis in respiratory disease. We undertook characterization of the prevalence of Pneumocystis and associated mucus in infant lungs.
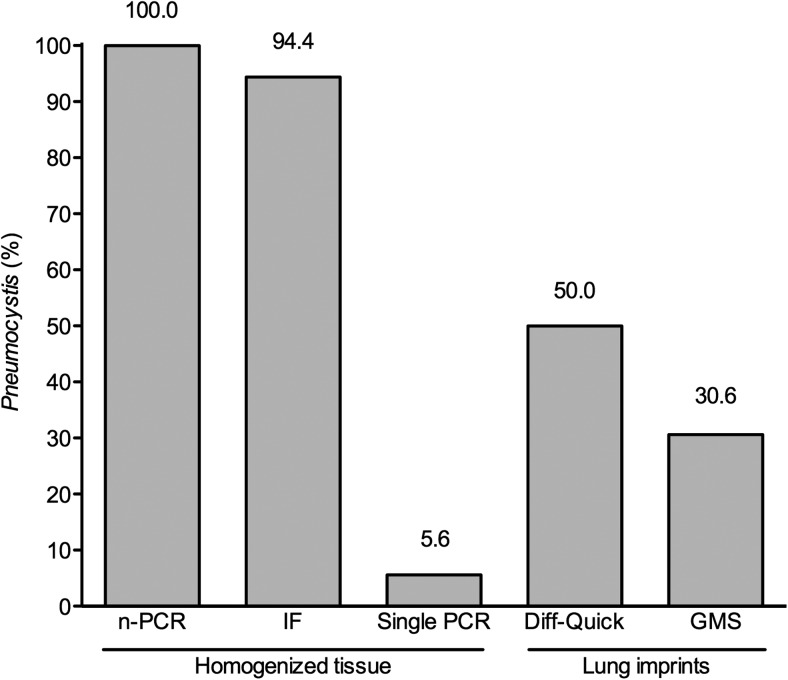
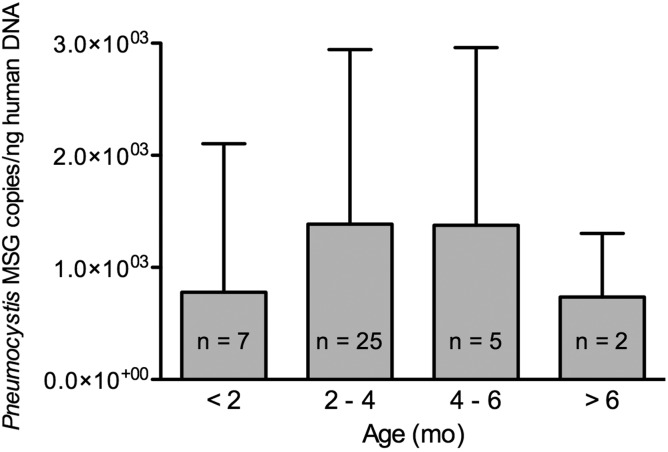
Methods: Samples from 128 infants (mean age, 101 days) who died suddenly and unexpectedly in Santiago during 1999-2004 were examined for Pneumocystis using nested polymerase chain reaction (nPCR) amplification of the P. jirovecii mtLSU ribosomal RNA gene and immunofluorescence microscopy (IF). Pneumocystis-negative infants 28 days and older and their age-closest positives were studied for MUC5AC expression and Pneumocystis burden by Western blot and quantitative PCR, respectively.
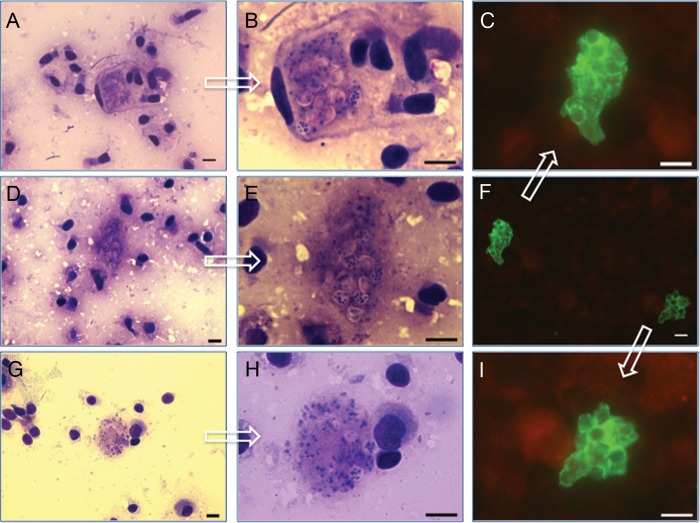
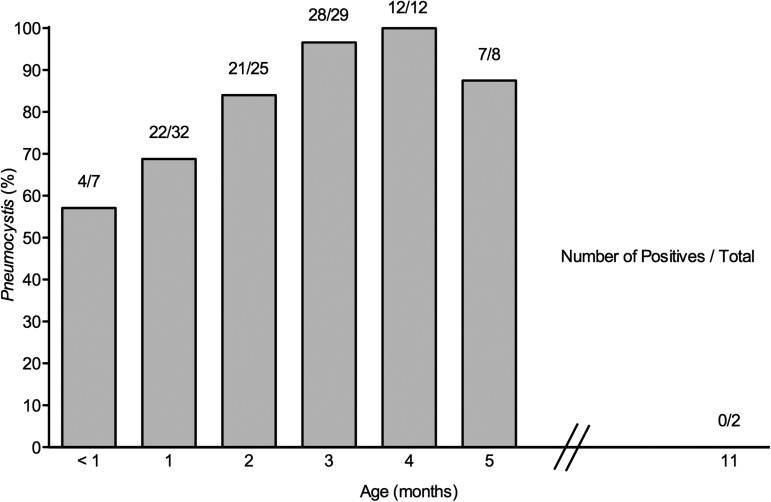
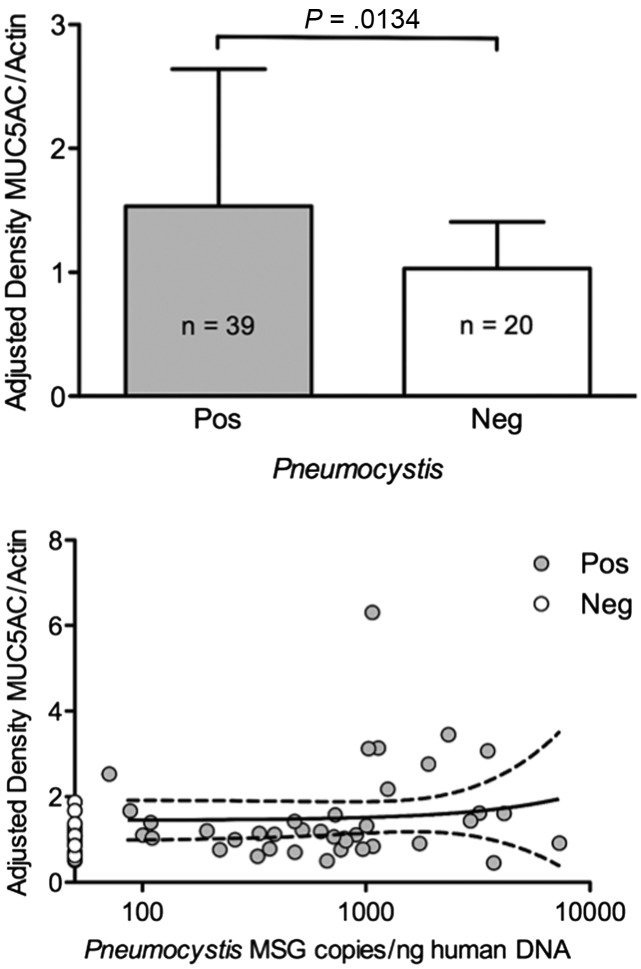
Results: Pneumocystis DNA was detected by nPCR in 105 of the 128 infants (82.0%) and Pneumocystis organisms were visualized by IF in 99 (94.3%) of the DNA-positive infants. The infection was commonest at 3-4 months with 40 of 41 (97.6%) infants of that age testing positive. MUC5AC was significantly increased in Pneumocystis-positive tissue specimens (P = .013). Death was unexplained in 113 (88.3%) infants; Pneumocystis was detected in 95 (84.0%) of them vs 10 of 15 (66.7%) with explained death (P = .28).
Conclusions: A highly focal Pneumocystis infection associated to increased mucus expression is almost universally present in the lungs of infants dying unexpectedly in the community regardless of autopsy diagnosis.
Figures
Comment in
-
Lung pathology associated with Pneumocystis colonization in infants.Clin Infect Dis. 2013 Jan;56(2):180-1. doi: 10.1093/cid/cis874. Epub 2012 Oct 16. Clin Infect Dis. 2013. PMID: 23074308 No abstract available.
References
-
- Vestereng VH, Bishop LR, Hernandez B, Kutty G, Larsen HH, Kovacs JA. Quantitative real-time polymerase chain-reaction assay allows characterization of Pneumocystis infection in immunocompetent mice. J Infect Dis. 2004;189:1540–4. - PubMed
-
- Soulez B, Dei-Cas E, Charet P, Mougeot G, Caillaux M, Camus D. The young rabbit: a nonimmunosuppressed model for Pneumocystis carinii pneumonia. J Infect Dis. 1989;160:355–6. - PubMed
-
- Vargas SL, Hughes WT, Santolaya ME, et al. Search for primary infection by Pneumocystis carinii in a cohort of normal, healthy infants. Clin Infect Dis. 2001;32:855–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
