

Pulmonary rehabilitation for patients with chronic pulmonary disease (COPD): an evidence-based analysis
- PMID: 23074434
- PMCID: PMC3384375
Pulmonary rehabilitation for patients with chronic pulmonary disease (COPD): an evidence-based analysis
Abstract
Objective: The objective of this evidence-based review was to determine the effectiveness and cost-effectiveness of pulmonary rehabilitation in the management of chronic obstructive pulmonary disease (COPD).
Technology: Pulmonary rehabilitation refers to a multidisciplinary program of care for patients with chronic respiratory impairment that is individually tailored and designed to optimize physical and social performance and autonomy. Exercise training is the cornerstone of pulmonary rehabilitation programs, though they may also include components such as patient education and psychological support. Pulmonary rehabilitation is recommended as the standard of care in the treatment and rehabilitation of patients with COPD who remain symptomatic despite treatment with bronchodilators.
For the purpose of this review, the Medical Advisory Secretariat focused on pulmonary rehabilitation programs as defined by the Cochrane Collaboration—that is, any inpatient, outpatient, or home-based rehabilitation program lasting at least 4 weeks that includes exercise therapy with or without any form of education and/or psychological support delivered to patients with exercise limitations attributable to COPD.
Research Questions:
What is the effectiveness and cost-effectiveness of pulmonary rehabilitation compared with usual care (UC) for patients with stable COPD?
Does early pulmonary rehabilitation (within 1 month of hospital discharge) in patients who had an acute exacerbation of COPD improve outcomes compared with UC (or no rehabilitation)?
Do maintenance or postrehabilitation programs for patients with COPD who have completed a pulmonary rehabilitation program improve outcomes compared with UC?
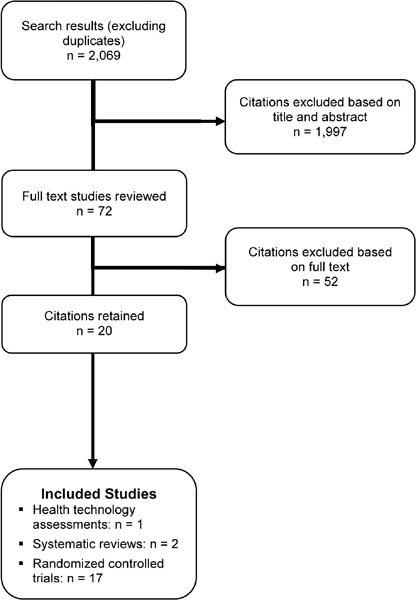
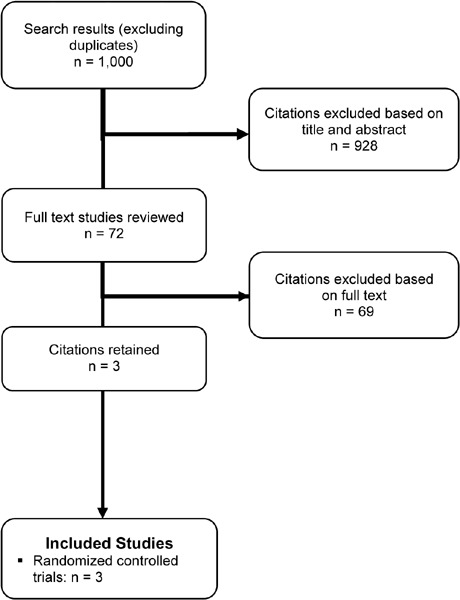
Search Strategy: For Research Questions 1and 2, a literature search was performed on August 10, 2010 for studies published from January 1, 2004 to July 31, 2010. For Research Question 3, a literature search was performed on February 3, 2011 for studies published from January 1, 2000 to February 3, 2011. Abstracts were reviewed by a single reviewer and, for those studies meeting the eligibility criteria, full-text articles were obtained. Reference lists and health technology assessment websites were also examined for any additional relevant studies not identified through the systematic search.
Inclusion Criteria: Research questions 1 and 2:
published between January 1, 2004 and July 31, 2010
randomized controlled trials, systematic reviews, and meta-analyses
COPD study population
studies comparing pulmonary rehabilitation with UC (no pulmonary rehabilitation)
duration of pulmonary rehabilitation program ≥ 6 weeks
pulmonary rehabilitation program had to include at minimum exercise training
Research question 3:
published between January 1, 2000 and February 3, 2011
randomized controlled trials, systematic reviews, and meta-analyses
COPD study population
studies comparing a maintenance or postrehabilitation program with UC (standard follow-up)
duration of pulmonary rehabilitation program ≥ 6 weeks
initial pulmonary rehabilitation program had to include at minimum exercise training
Exclusion Criteria: Research questions 1, 2, and 3:
grey literature
duplicate publications
non-English language publications
study population ≤ 18 years of age
studies conducted in a palliative population
studies that did not report primary outcome of interest
Additional exclusion criteria for research question 3:
studies with ≤ 2 sessions/visits per month
Outcomes of Interest: The primary outcomes of interest for the stable COPD population were exercise capacity and health-related quality of life (HRQOL). For the COPD population following an exacerbation, the primary outcomes of interest were hospital readmissions and HRQOL. The primary outcomes of interest for the COPD population undertaking maintenance programs were functional exercise capacity and HRQOL.
Quality of Evidence: The quality of each included study was assessed taking into consideration allocation concealment, randomization, blinding, power/sample size, withdrawals/dropouts, and intention-to-treat analyses.
The quality of the body of evidence was assessed as high, moderate, low, or very low according to the GRADE Working Group criteria. The following definitions of quality were used in grading the quality of the evidence:
[Table: see text]
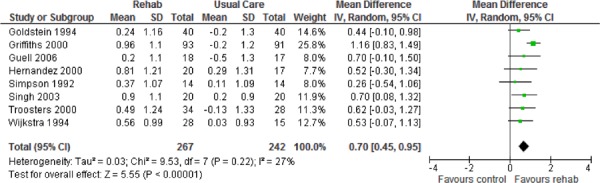
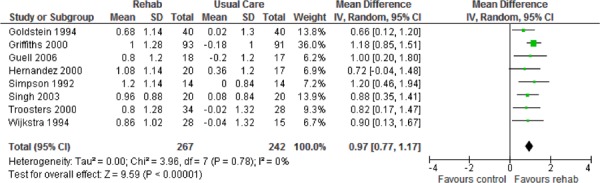
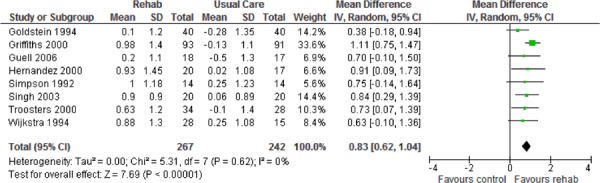
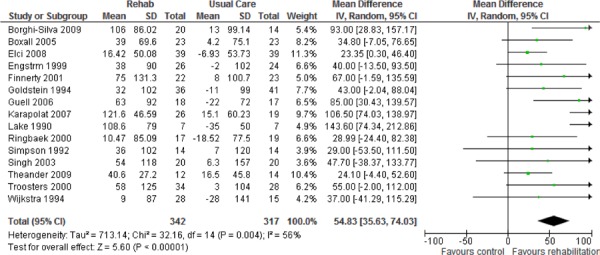
Research Question 1: Effect of Pulmonary Rehabilitation on Outcomes in Stable COPD: Seventeen randomized controlled trials met the inclusion criteria and were included in this review.
The following conclusions are based on moderate quality of evidence.
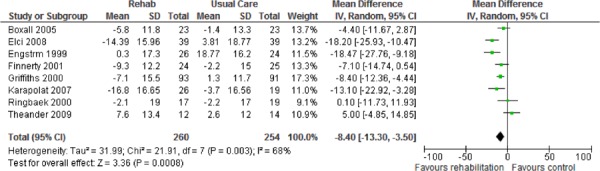
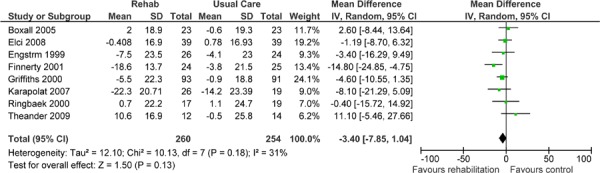
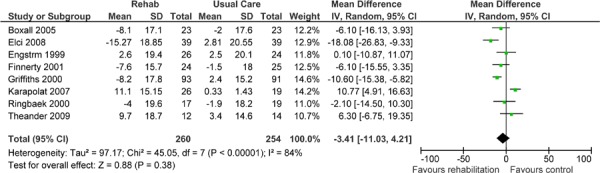
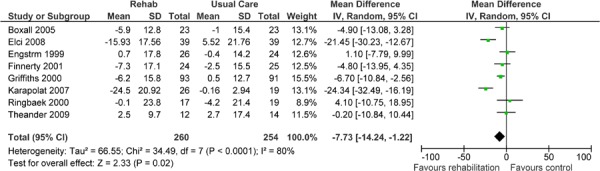
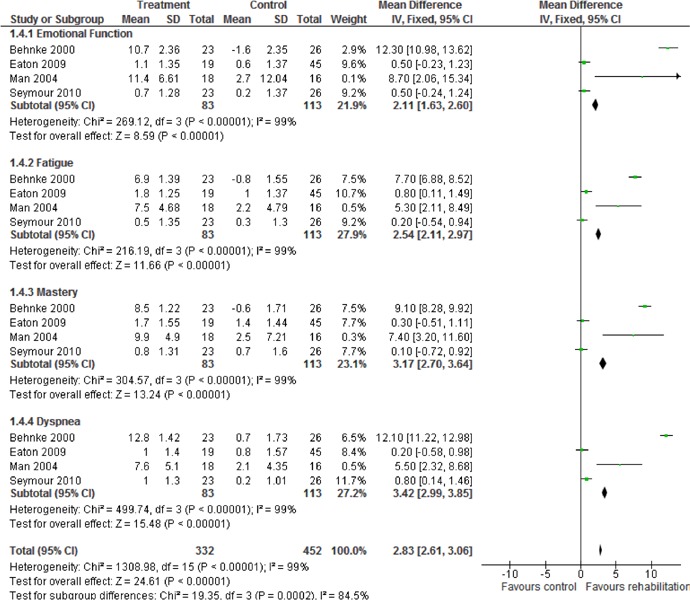
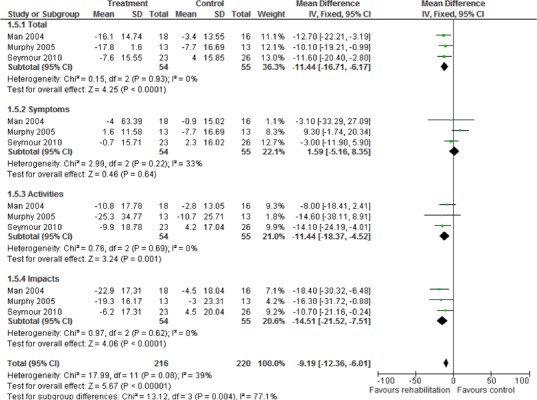
Pulmonary rehabilitation including at least 4 weeks of exercise training leads to clinically and statistically significant improvements in HRQOL in patients with COPD.
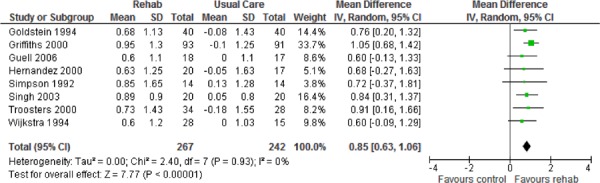
Pulmonary rehabilitation also leads to a clinically and statistically significant improvement in functional exercise capacity (weighted mean difference, 54.83 m; 95% confidence interval, 35.63–74.03; P < 0.001).
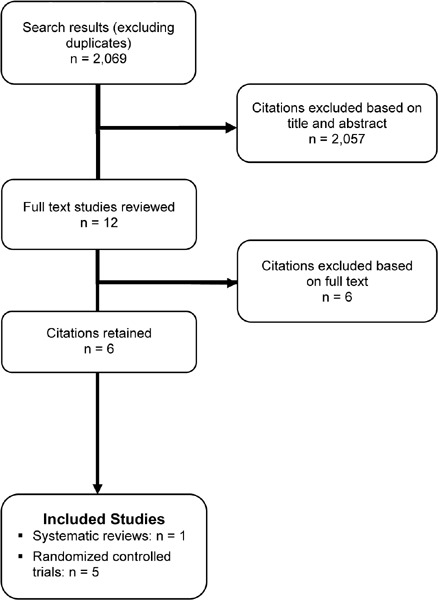
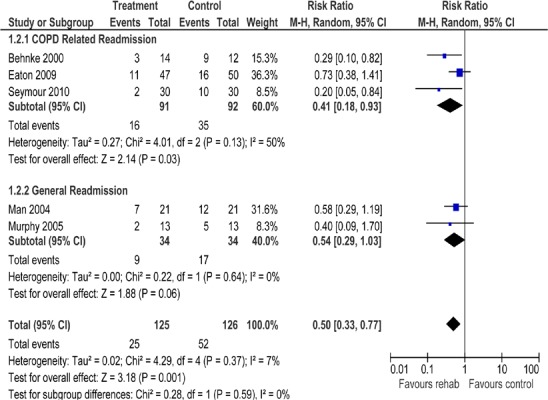
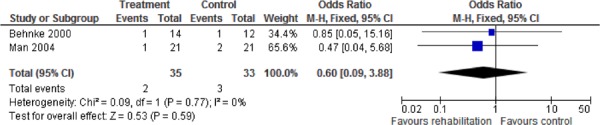
Research Question 2: Effect of Pulmonary Rehabilitation on Outcomes Following an Acute Exacerbation of COPD: Five randomized controlled trials met the inclusion criteria and are included in this review. The following conclusion is based on moderate quality of evidence.
Pulmonary rehabilitation (within 1 month of hospital discharge) after acute exacerbation significantly reduces hospital readmissions (relative risk, 0.50; 95% confidence interval, 0.33–0.77; P = 0.001) and leads to a statistically and clinically significant improvement in HRQOL.
Research Question 3: Effect of Pulmonary Rehabilitation Maintenance Programs on COPD Outcomes: Three randomized controlled trials met the inclusion criteria and are included in this review. The conclusions are based on a low quality of evidence and must therefore be considered with caution.
Maintenance programs have a nonsignificant effect on HRQOL and hospitalizations.
Maintenance programs have a statistically but not clinically significant effect on exercise capacity (P = 0.01). When subgrouped by intensity and quality of study, maintenance programs have a statistically and marginally clinically significant effect on exercise capacity.
Figures



References
-
- Lacasse Y, Maltais F, Goldstein RS. Smoking cessation in pulmonary rehabilitation: goal or prerequisite? J Cardpulm Rehabil. 2002 May;22(3):148–53. - PubMed
-
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Wantanabe N. Imputing missing standard deviations in meta-analyses can provide accurate results. J Clin Epidemiol. 2006 Jan 1;59(1):7–10. - PubMed
-
- Thiessen PH, Barrowman N, Garg AX. Imputing variance estimates do not alter the conclusions of a meta-analysis with continuous outcomes: a case study of changes in renal function after living kidney donation. J Clin Epidemiol. 2007 Jan 1;60(3):228–40. - PubMed
-
- Goodman C. Literature searching and evidence interpretation for assessing health care practices. Stockholm, Sweden: Swedish Council on Technology Assessment in Health Care. SBU Report No. 119E. 1996 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous