

Ultrasound screening for abdominal aortic aneurysm: an evidence-based analysis
- PMID: 23074490
- PMCID: PMC3379169
Ultrasound screening for abdominal aortic aneurysm: an evidence-based analysis
Abstract
Objective: The aim of this review was to assess the effectiveness of ultrasound screening for asymptomatic abdominal aortic aneurysm (AAA).
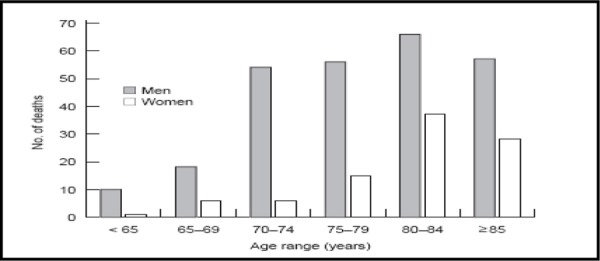
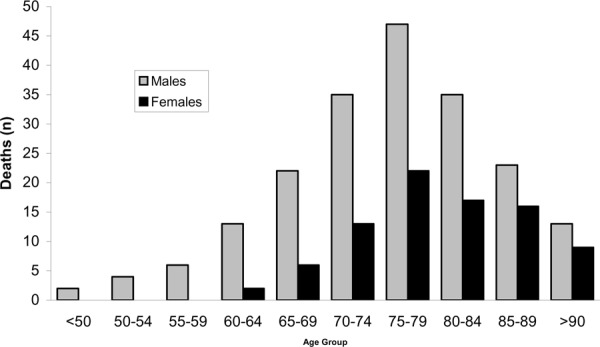
Clinical need: Abdominal aortic aneurysm is a localized abnormal dilatation of the aorta greater than 3 cm. In community surveys, the prevalence of AAA is reported to be between 2% and 5.4%. Abdominal aortic aneurysms are found in 4% to 8% of older men and in 0.5% to 1.5% of women aged 65 years and older. Abdominal aortic aneurysms are largely asymptomatic. If left untreated, the continuing extension and thinning of the vessel wall may eventually result in rupture of the AAA. Often rupture may occur without warning, causing acute pain. Rupture is always life threatening and requires emergency surgical repair of the ruptured aorta. The risk of death from ruptured AAA is 80% to 90%. Over one-half of all deaths attributed to a ruptured aneurysm take place before the patient reaches hospital. In comparison, the rate of death in people undergoing elective surgery is 5% to 7%; however, symptoms of AAA rarely occur before rupture. Given that ultrasound can reliably visualize the aorta in 99% of the population, and its sensitivity and specificity for diagnosing AAA approaches 100%, screening for aneurysms is worth considering as it may reduce the incidence of ruptured aneurysms and hence reduce unnecessary deaths caused by AAA-attributable mortality.
Review strategy: The Medical Advisory Secretariat used its standard search strategy to retrieve international health technology assessments and English-language journal articles from selected databases to determine the effectiveness of ultrasound screening for abdominal aortic aneurysms. Case reports, letters, editorials, nonsystematic reviews, non-human studies, and comments were excluded. Questions asked: Is population-based AAA screening effective in improving health outcomes in asymptomatic populations?Is AAA screening acceptable to the population? Does this affect the effectiveness the screening program?How often should population-based screening occur?What are appropriate treatment options after screening based on the size of aneurysms?Are there differences between universal and targeted screening strategies?What are the harms of screening?
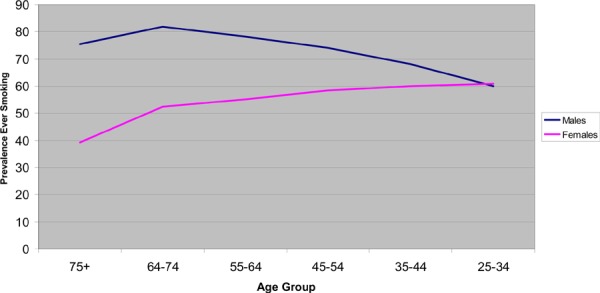
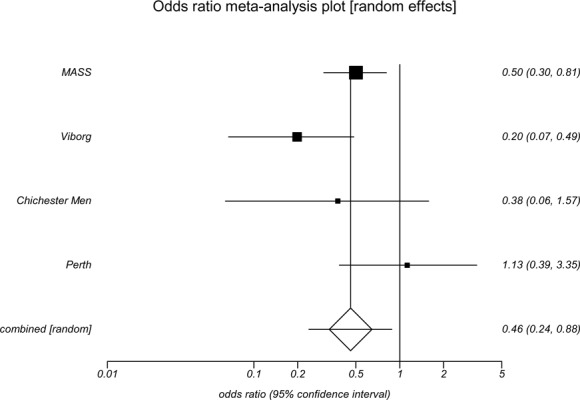
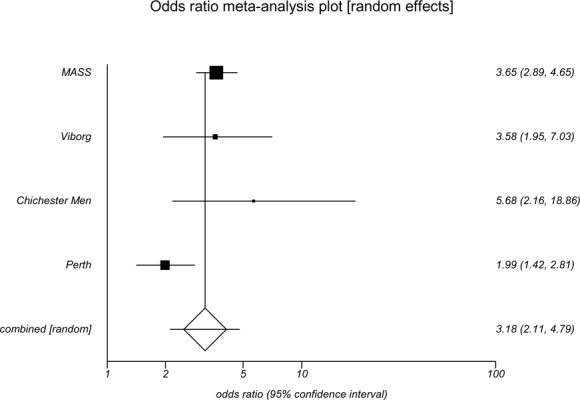
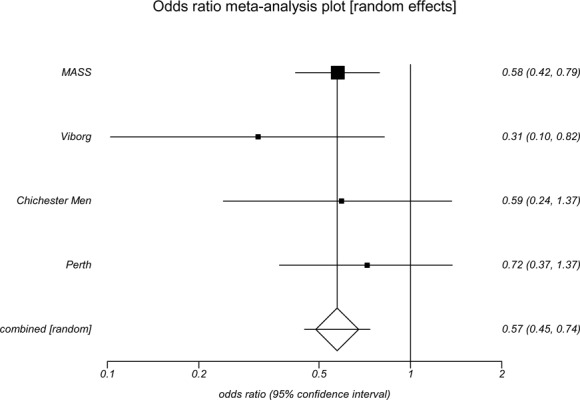
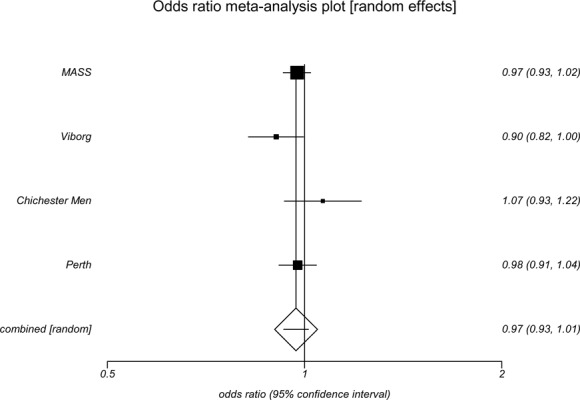
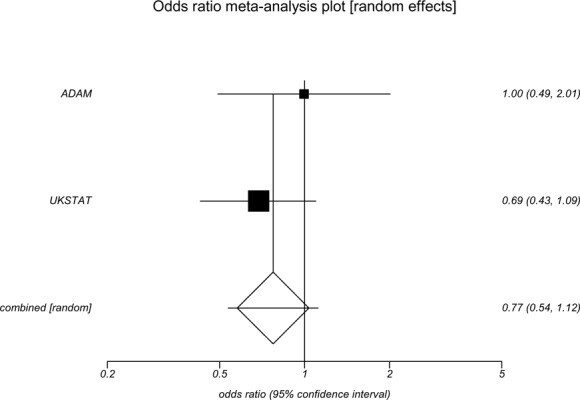
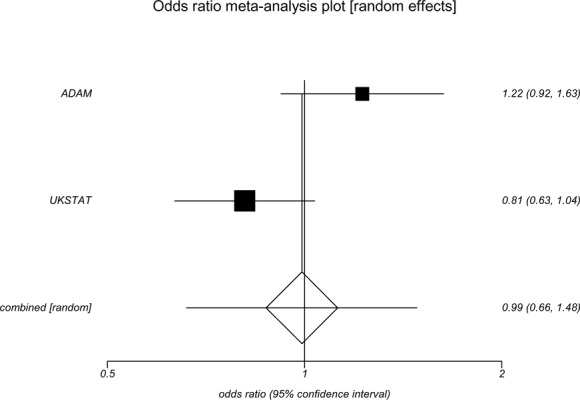
Summary of findings: Population-based ultrasound screening is effective in men aged 65 to 74 years, particularly in those with a history of smoking. Screening reduces the incidence of AAA ruptures, and decreases rates of emergency surgical repair for AAA and AAA-attributable mortality.Acceptance rates decline with increasing age and are lower for women. Low acceptance rates may affect the effectiveness of a screening program.A one-time screen is sufficient for a population-based screening program with regard to initial negative scans and development of large AAAs.There is no difference between early elective surgical repair and surveillance for small aneurysms (4.0-5.4 cm). Repeated surveillance of small aneurysms is recommended.Targeted screening based on history of smoking has been found to detect 89% of prevalent AAAs and increase the efficiency of screening programs from statistical modeling data.Women have not been studied for AAA screening programs. There is evidence suggesting that screening women for AAA should be considered with respect to mortality and case fatality rates in Ontario. It is important that further evaluation of AAAs in women occur.There is a small risk of physical harm from screening. Less than 1% of aneurysms will not be visualized on initial screen and a re-screen may be necessary; elective surgical repair is associated with a 6% operative morality rate and about 3% of small aneurysms may rupture during surveillance. These risks should be communicated through informed consent prior to screening.There is little evidence of severe psychological harms associated with screening.
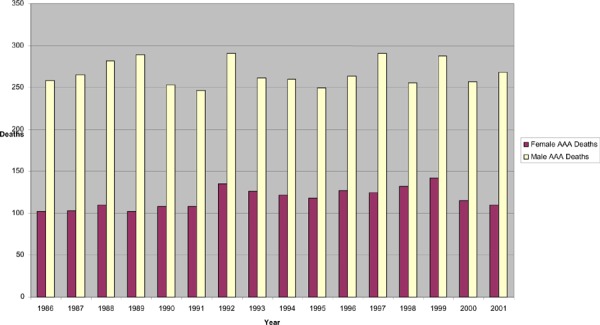
Conclusions: Based on this review, the Medical Advisory Secretariat concluded that there is sufficient evidence to determine that AAA screening using ultrasound is effective and reduces negative health outcomes associated with the condition. Moreover, screening for AAA is cost-effective, comparing favorably for the cost of per life year gained for screening programs for cervical cancer, hypertension, and breast cancer that are in practice in Ontario, with a high degree of compliance, and can be undertaken with a minimal effort at fewer than 10 minutes to screen each patient. Overall, the clinical utility of an invitation to use ultrasound screening to identify AAA in men aged 65 to 74 is effective at reducing AAA-attributable mortality. The benefit of screening women is not yet established. However, Ontario data indicate several areas of concern including population prevalence, detection of AAA in women, and case management of AAA in women in terms of age cutoffs for screening and natural history of disease associated with age of rupture.
Figures
Similar articles
-
Endovascular repair of abdominal aortic aneurysm: an evidence-based analysis.Ont Health Technol Assess Ser. 2002;2(1):1-46. Epub 2002 Mar 1. Ont Health Technol Assess Ser. 2002. PMID: 23074438 Free PMC article.
-
Primary Care Screening for Abdominal Aortic Aneurysm: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Dec. Report No.: 19-05253-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Dec. Report No.: 19-05253-EF-1. PMID: 31877008 Free Books & Documents. Review.
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Screening women aged 65 years or over for abdominal aortic aneurysm: a modelling study and health economic evaluation.Health Technol Assess. 2018 Aug;22(43):1-142. doi: 10.3310/hta22430. Health Technol Assess. 2018. PMID: 30132754 Free PMC article.
-
Primary Care Screening for Abdominal Aortic Aneurysm: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force.JAMA. 2019 Dec 10;322(22):2219-2238. doi: 10.1001/jama.2019.17021. JAMA. 2019. PMID: 31821436
Cited by
-
Identification of the main determinants of abdominal aorta size: a screening by Pocket Size Imaging Device.Cardiovasc Ultrasound. 2017 Jan 13;15(1):2. doi: 10.1186/s12947-016-0094-z. Cardiovasc Ultrasound. 2017. PMID: 28086907 Free PMC article.
-
Screening Tool to Identify Patients with Advanced Aortic Valve Stenosis.J Clin Med. 2022 Jul 28;11(15):4386. doi: 10.3390/jcm11154386. J Clin Med. 2022. PMID: 35956007 Free PMC article.
-
The Role of Imaging in Health Screening: Screening for Specific Conditions.Acad Radiol. 2021 Apr;28(4):548-563. doi: 10.1016/j.acra.2020.03.039. Epub 2020 May 11. Acad Radiol. 2021. PMID: 32404272 Free PMC article. Review.
-
Screening for abdominal aortic aneurysms in Canada: 2020 review and position statement of the Canadian Society for Vascular Surgery.Can J Surg. 2021 Sep 1;64(5):E461-E466. doi: 10.1503/cjs.009120. Can J Surg. 2021. PMID: 34467750 Free PMC article. Review.
-
Screening for abdominal aortic aneurysm.Can Fam Physician. 2012 Mar;58(3):253. Can Fam Physician. 2012. PMID: 22423019 Free PMC article. No abstract available.
References
-
- Braunwald E, Fauci AS, Kasper DL, Hauser S, Longo DL, Jameson JL. 15th ed. New York: McGraw-Hill; 2001. Harrison’s principles of internal medicine.
-
- Patterson C Canadian Task Force on Preventative Health Care. Screening for abdominal aortic aneurysms [monograph on the Internet] Ottawa: Health Canada. 1994. [[cited 2004 Oct. 10]]. pp. 672–678. Available from: http://www.ctfphc.org/Full_Text/Ch55full.htm .
-
- Heller JA, Weinberg A, Arons R, Krishnanastry KV, Lyon RT, Deitch JS, et al. Two decades of aneurysmal repair: have we made any progress? J Vasc Surg. 2005;32(6):1091–1100. - PubMed
-
- Hallett JW Jr. Management of abdominal aortic aneurysms. Mayo Clin Proc. 2000;75(4):395–399. - PubMed
-
- Fleming C, Whitlock EP, Beil TL, Lederle FA. Screening for abdominal aortic aneurysm: a best-evidence systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2005;142(3):203–211. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials