

Dose optimization for near-infrared fluorescence sentinel lymph node mapping in patients with melanoma
- PMID: 23078649
- PMCID: PMC3607940
- DOI: 10.1111/bjd.12059
Dose optimization for near-infrared fluorescence sentinel lymph node mapping in patients with melanoma
Abstract
Background: Regional lymph node involvement is the most important prognostic factor in cutaneous melanoma. As only 20% of patients with melanoma have occult nodal disease and would benefit from a regional lymphadenectomy, the sentinel lymph node (SLN) biopsy was introduced. Near-infrared (NIR) fluorescence has been hypothesized to improve SLN mapping.
Objectives: To assess the potential of intraoperative NIR fluorescence imaging to improve SLN mapping in patients with melanoma and to examine the optimal dose of indocyanine green adsorbed to human serum albumin (ICG:HSA).
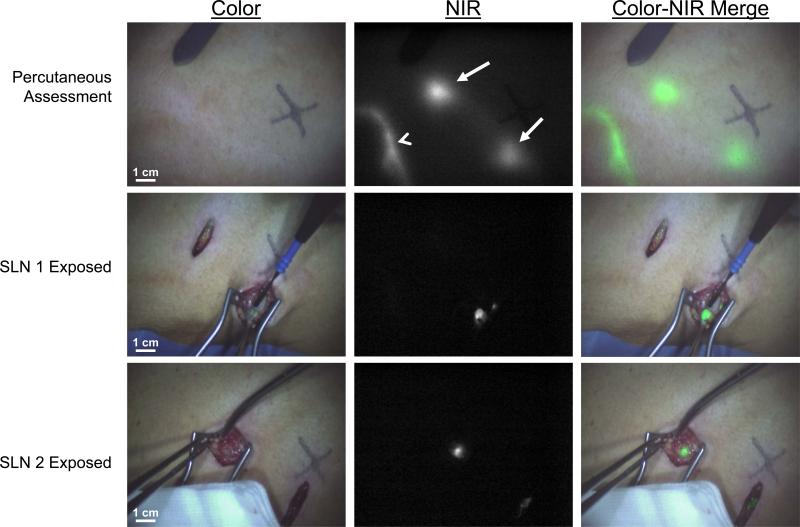
Methods: Fifteen consecutive patients with cutaneous melanoma underwent the standard SLN procedure using (99m) technetium-nancolloid and patent blue. In addition, intraoperative NIR fluorescence imaging was performed after injection of 1·6 mL of 600, 800, 1000 or 1200 μmolL(-1) of ICG: HSA in four quadrants around the primary excision scar.
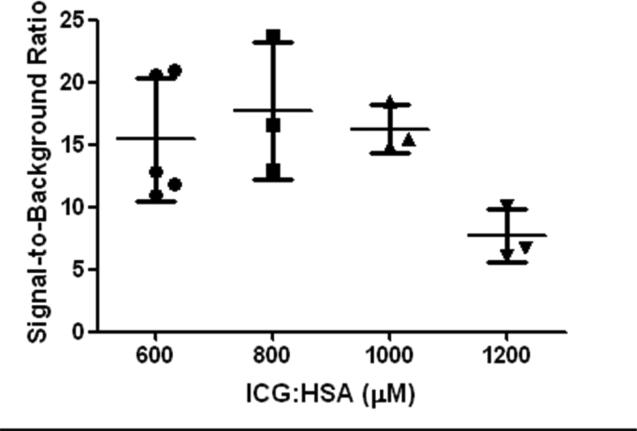
Results: NIR fluorescence SLN mapping was successful in 93% of patients. In one patient, no SLN could be identified using either conventional methods or NIR fluorescence. A total of 30 SLNs (average 2·0, range 1-7) were detected, 30 radioactive (100%), 27 blue (73%) and 30 NIR fluorescent (100%). With regard to the effect of concentration on signal-to-background ratios a trend (P=0·066) was found favouring the 600, 800 and 1000 μmol L(-1) groups over the 1200 μmol L(-1) group.
Conclusion: This study demonstrates feasibility and accuracy of SLN mapping using ICG: HSA. Considering safety, cost and pharmacological characteristics, an ICG: HSA concentration of 600 μmolL(-1) appears optimal for SLN mapping in cutaneous melanoma, although lower doses need to be assessed.
© 2012 The Authors. BJD © 2012 British Association of Dermatologists.
Figures
References
-
- Balch CM, Soong SJ, Atkins MB, et al. An evidence-based staging system for cutaneous melanoma. CA Cancer J Clin. 2004;54:131–49. - PubMed
-
- Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392–9. - PubMed
-
- Thompson JF, McCarthy WH, Bosch CM, et al. Sentinel lymph node status as an indicator of the presence of metastatic melanoma in regional lymph nodes. Melanoma Res. 1995;5:255–60. - PubMed
-
- Gershenwald JE, Ross MI. Sentinel-lymph-node biopsy for cutaneous melanoma. N Engl J Med. 2011;364:1738–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
