An intervention to improve cause-of-death reporting in New York City hospitals, 2009-2010
- PMID: 23078668
- PMCID: PMC3477897
- DOI: 10.5888/pcd9.120071
An intervention to improve cause-of-death reporting in New York City hospitals, 2009-2010
Abstract
Introduction: Poor-quality cause-of-death reporting reduces reliability of mortality statistics used to direct public health efforts. Overreporting of heart disease has been documented in New York City (NYC) and nationwide. Our objective was to evaluate the immediate and longer-term effects of a cause-of-death (COD) educational program that NYC's health department conducted at 8 hospitals on heart disease reporting and on average conditions per certificate, which are indicators of the quality of COD reporting.
Methods: From June 2009 through January 2010, we intervened at 8 hospitals that overreported heart disease deaths in 2008. We shared hospital-specific data on COD reporting, held conference calls with key hospital staff, and conducted in-service training. For deaths reported from January 2009 through June 2011, we compared the proportion of heart disease deaths and average number of conditions per death certificate before and after the intervention at both intervention and nonintervention hospitals.
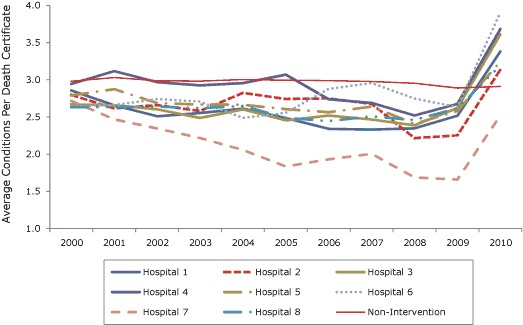
Results: At intervention hospitals, the proportion of death certificates that reported heart disease as the cause of death decreased from 68.8% preintervention to 32.4% postintervention (P < .001). Individual hospital proportions ranged from 58.9% to 79.5% preintervention and 25.9% to 45.0% postintervention. At intervention hospitals the average number of conditions per death certificate increased from 2.4 conditions preintervention to 3.4 conditions postintervention (P < .001) and remained at 3.4 conditions a year later. At nonintervention hospitals, these measures remained relatively consistent across the intervention and postintervention period.
Conclusion: This NYC health department's hospital-level intervention led to durable changes in COD reporting.
Figures

References
-
- Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death certificates for coding coronary heart disease as the cause of death. Ann Intern Med 1998;129(12):1020–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical