

Successful clinical outcomes following decentralization of tertiary paediatric HIV care to a community-based paediatric antiretroviral treatment network, Chiangrai, Thailand, 2002 to 2008
- PMID: 23078768
- PMCID: PMC3494174
- DOI: 10.7448/IAS.15.2.17358
Successful clinical outcomes following decentralization of tertiary paediatric HIV care to a community-based paediatric antiretroviral treatment network, Chiangrai, Thailand, 2002 to 2008
Abstract
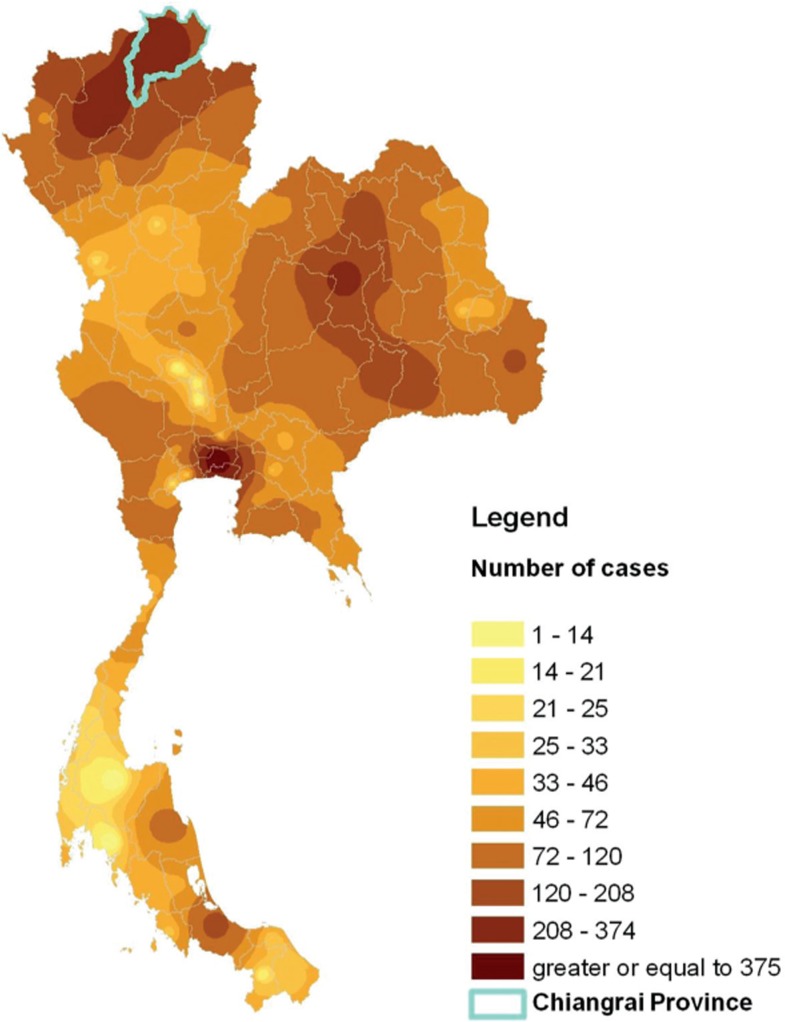
Introduction: Most paediatric antiretroviral treatments (ARTs) in Thailand are limited to tertiary care hospitals. To decentralize paediatric HIV treatment and care, Chiangrai Prachanukroh Hospital (CRH) strengthened a provincial paediatric HIV care network by training community hospital (CH) care teams to receive referrals of children for community follow-up. In this study, we assessed factors associated with death and clinical outcomes of HIV-infected children who received care at CRH and CHs after implementation of a community-based paediatric HIV care network.
Methods: Clinical records were abstracted for all children who initiated ART at CRH. Paired Wilcoxon signed rank tests were used to assess CD4% and virological change among all children. Cox proportional hazard models were used to assess factors associated with death. Treatment outcomes (CD4%, viral load (VL) and weight-for-age Z-score (WAZ)) were compared between CRH and CH children who met the criteria for analysis.
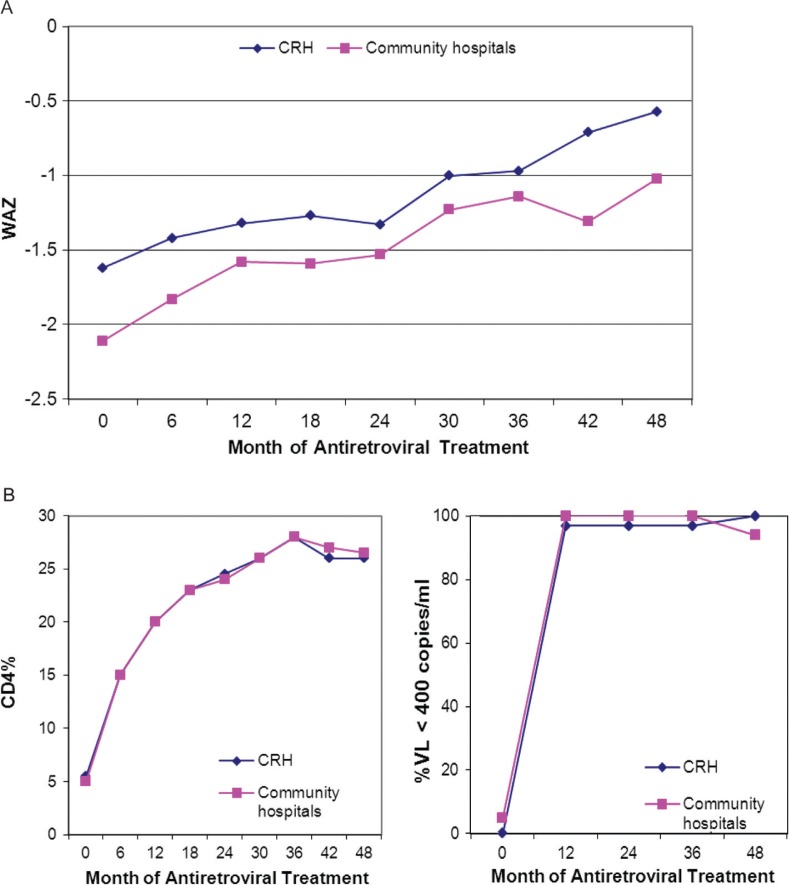
Results: Between February 2002 and April 2008, 423 HIV-infected children initiated ART and 410 included in the cohort analysis. Median follow-up for the cohort was 28 months (interquartile range (IQR)=12 to 42); 169 (41%) children were referred for follow-up at CH. As of 31 March 2008, 42 (10%) children had died. Baseline WAZ (< -2 (p=0.001)) and baseline CD4% (<5% (p=0.015)) were independently associated with death. At 48 months, 86% of ART-naïve children in follow-up had VL<400 copies/ml. For sub-group analysis, 133 children at CRH and 154 at CHs were included for comparison. Median baseline WAZ was lower in CH children than in CRH children (p=0.001); in both groups, WAZ, CD4% and VL improved after ART with no difference in rate of WAZ and CD4% gain (p=0.421 and 0.207, respectively).
Conclusions: Children at CHs had more severe immunological suppression and low WAZ at baseline. Community- and tertiary care-based paediatric ART follow-ups result in equally beneficial outcomes with the strengthening of a provincial referral network between tertiary and community care. Nutrition interventions may benefit children in community-based HIV treatment and care.
Figures

References
-
- Global HIV/AIDS response epidemic update and health sector progress towards Universal Access progress report 2011. WHO, UNAIDS, UNICEF. accessed 2012 January 19 Available from: http://www.who.int/hiv/pub/progress_report2011/summary_en.pdf.
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364:1236–43. - PubMed
-
- Brahmbhatt H, Kigozi G, Wabwire-Mangen F, Serwadda D, Lutalo T, Nalugoda F, et al. Mortality in HIV-infected and uninfected children of HIV-infected and uninfected mothers in rural Uganda. J Acquir Immune Defic Syndr. 2006;41:504–8. - PubMed
-
- Gortmaker SL, Hughes M, Cervia J, Brady M, Johnson GM, Seage GR, 3rd, et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001;345:1522–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
