

A comparison of RIFLE with and without urine output criteria for acute kidney injury in critically ill patients
- PMID: 23078781
- PMCID: PMC3682302
- DOI: 10.1186/cc11808
A comparison of RIFLE with and without urine output criteria for acute kidney injury in critically ill patients
Abstract
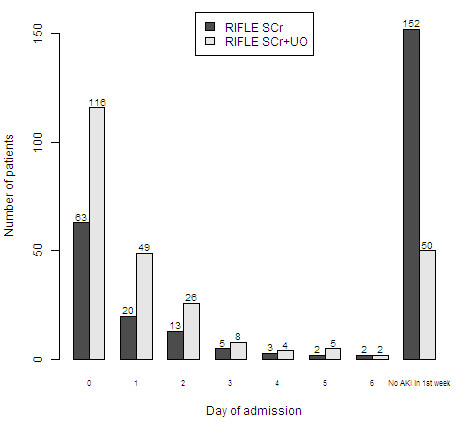
Introduction: The Risk, Injury, Failure, Loss, and End-Stage Renal Disease (RIFLE) is a consensus-based classification system for diagnosing acute kidney insufficiency (AKI), based on serum creatinine (SCr) and urine output criteria (RIFLESCr+UO). The urine output criteria, however, are frequently discarded and many studies in the literature applied only the SCr criteria (RIFLESCr). We diagnosed AKI using both RIFLE methods and compared the effects on time to AKI diagnosis, AKI incidence and AKI severity.
Methods: This was a prospective observational cohort study during four months in adult critically ill patients admitted to the ICU for at least 48 hours. During the first week patients were scored daily for AKI according to RIFLESCr+UO and RIFLESCr. We assessed urine output hourly and fluid balance daily. The baseline SCr was estimated if a recent pre-ICU admission SCr was unknown. Based on the two RIFLE methods for each patient we determined time to AKI diagnosis (AKI-0) and maximum RIFLE grade.
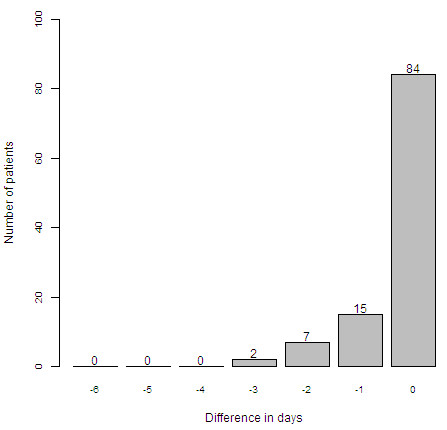
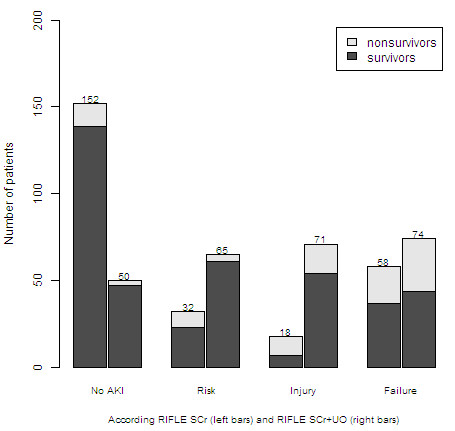
Results: We studied 260 patients. A pre-ICU admission SCr was available in 101 (39%) patients. The two RIFLE methods resulted in statistically significantly different outcomes for incidence of AKI, diagnosis of AKI for individual patients, distribution of AKI-0 and distribution of the maximum RIFLE grade. Discarding the RIFLE urine criteria for AKI diagnosis significantly underestimated the presence and grade of AKI on admission and during the first ICU week (P < 0,001) and significantly delayed the diagnosis of AKI (P < 0.001). Based on RIFLESCr 45 patients had no AKI on admission but subsequently developed AKI. In 24 of these patients (53%) AKI would have been diagnosed at least one day earlier if the RIFLE urine criteria had been applied. Mortality rate in the AKI population was 38% based on RIFLESCr and 24% based on RIFLESCr+UO (P = 0.02).
Conclusions: The use of RIFLE without the urine criteria significantly underscores the incidence and grade of AKI, significantly delays the diagnosis of AKI and is associated with higher mortality.
Figures
Comment in
-
RIFLE is alive: long live RIFLE.Crit Care. 2012 Nov 29;16(6):182. doi: 10.1186/cc11851. Crit Care. 2012. PMID: 23190722 Free PMC article.
-
Comparison of RIFLE with and without urine output criteria for acute kidney injury in critically ill patients: a task still not concluded!Crit Care. 2013 Jan 23;17(1):408. doi: 10.1186/cc11911. Crit Care. 2013. PMID: 23343459 Free PMC article. No abstract available.
-
Authors' response.Crit Care. 2013;17(1):408. Crit Care. 2013. PMID: 25215364 No abstract available.
References
-
- Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;16:819–825. - PubMed
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;16:R204–R212. doi: 10.1186/cc2872. - DOI - PMC - PubMed
-
- Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;16:461–470. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
