

Endoscopic full-thickness biopsy of the gastric wall with defect closure by using an endoscopic suturing device: survival porcine study
- PMID: 23078926
- PMCID: PMC3666864
- DOI: 10.1016/j.gie.2012.07.010
Endoscopic full-thickness biopsy of the gastric wall with defect closure by using an endoscopic suturing device: survival porcine study
Abstract
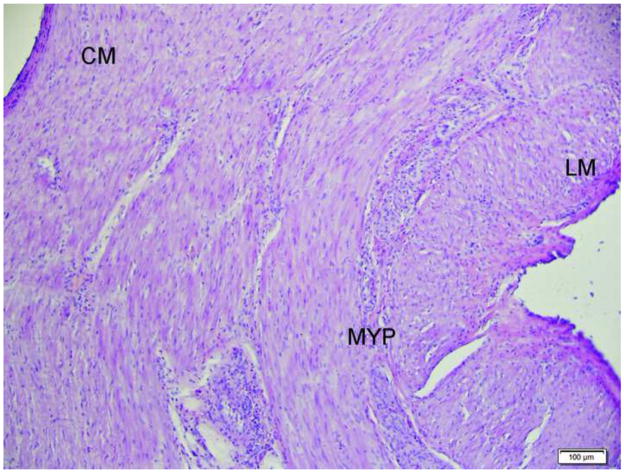
Background: The pathogenesis of several common gastric motility diseases and functional GI disorders remains essentially unexplained. Gastric wall biopsies that include the muscularis propria to evaluate the enteric nervous system, interstitial cells of Cajal, and immune cells can provide important insights for our understanding of the etiology of these disorders.
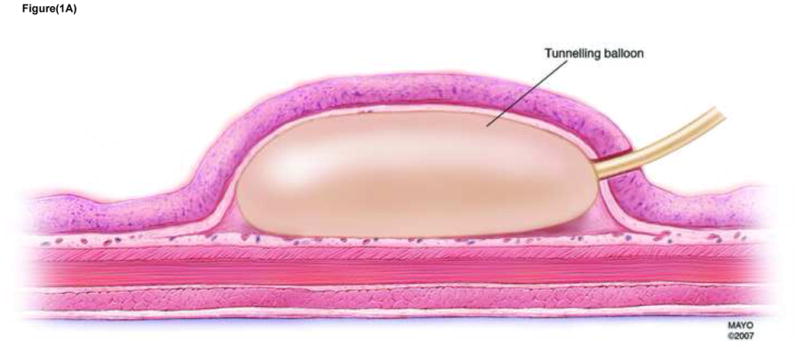
Objectives: To determine the technical feasibility, reproducibility, and safety of performing a full-thickness gastric biopsy (FTGB) by using a submucosal endoscopy with mucosal flap (SEMF) technique; the technical feasibility, reproducibility, and safety of tissue closure by using an endoscopic suturing device; the ability to identify myenteric ganglia in resected specimens; and the long-term safety.
Design: Single center, preclinical survival study.
Setting: Animal research laboratory, developmental endoscopy unit.
Subjects: Twelve domestic pigs.
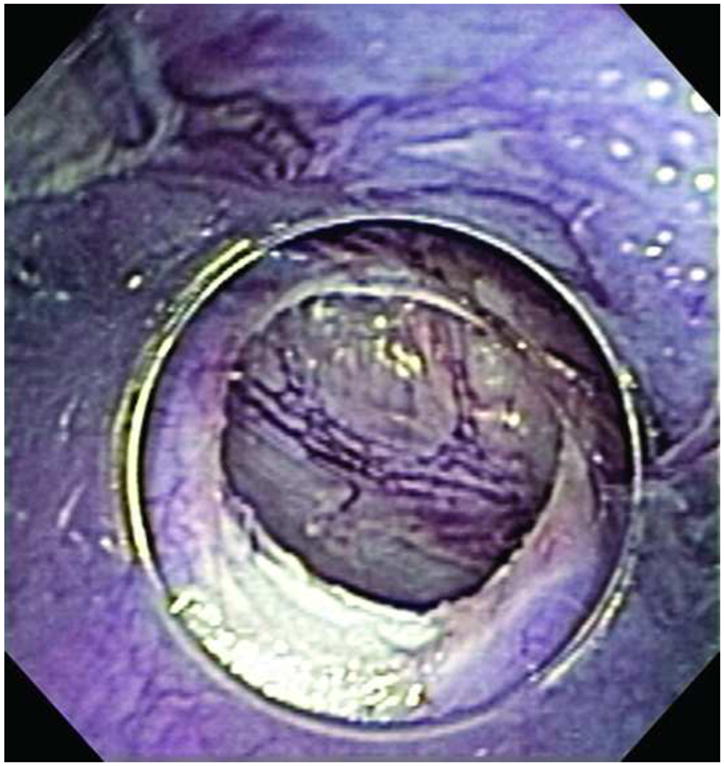
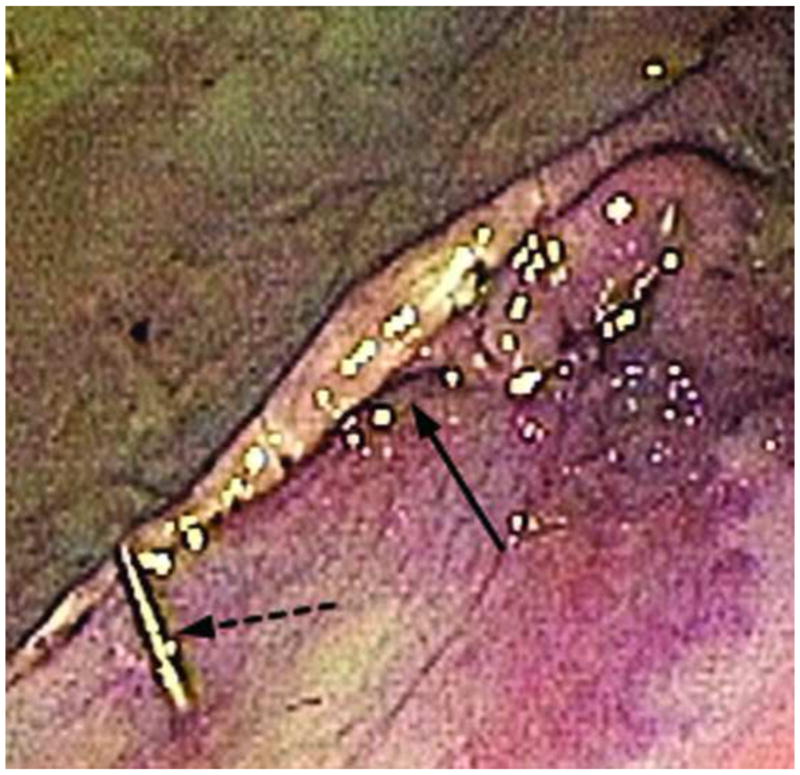
Interventions: Animals underwent an SEMF procedure with gastric muscularis propria resection. The resultant offset mucosal entry site was closed by using an endoscopic suturing device. Animals were kept alive for 2 weeks.
Main outcome measurements: The technical feasibility, reproducibility, and safety of the procedure; the clinical course of the animals; the histological and immunochemical evaluation of the resected specimen to determine whether myenteric ganglia were present in the sample.
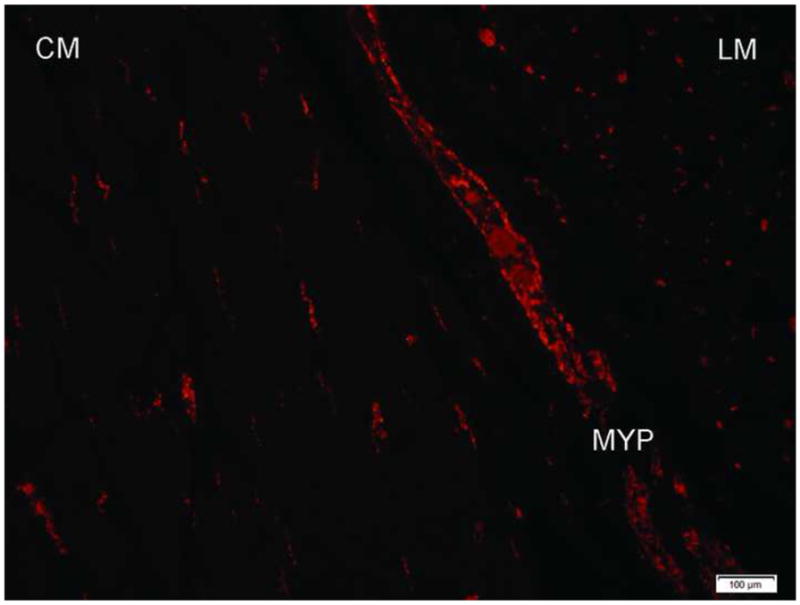
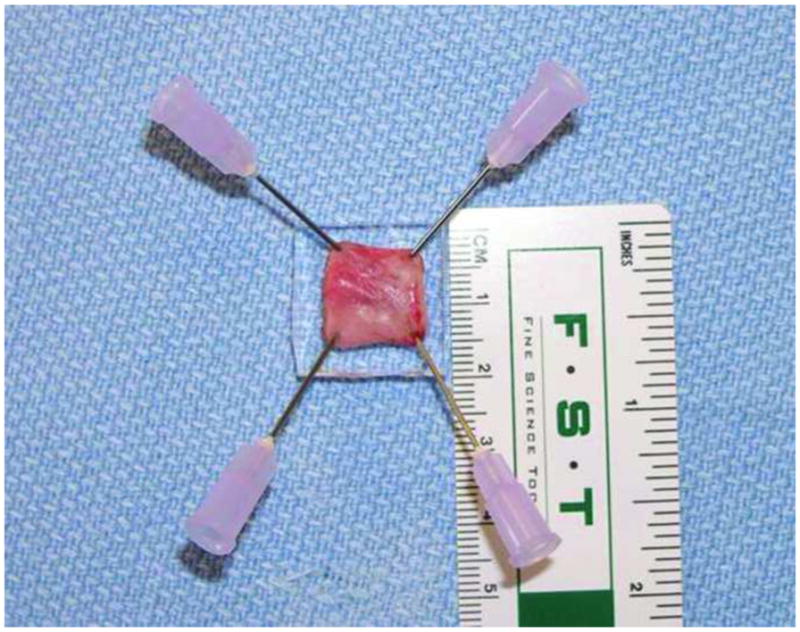
Results: FTGB was performed by using the SEMF technique in all 12 animals. The offset mucosal entry site was successfully closed by using the suturing device in all animals. The mean resected tissue specimen size was 11 mm. Mean total procedure time was 61 minutes with 2 to 4 interrupted sutures placed per animal. Histology showed muscularis propria and serosa, confirming full-thickness resections in all animals. Myenteric ganglia were visualized in 11 of 12 animals. The clinical course was uneventful. Repeat endoscopy and necropsy at 2 weeks showed absence of ulceration at both the mucosal entry sites and overlying the more distal muscularis propria resection sites. There was complete healing of the serosa in all animals with minimal single-band adhesions in 5 of 12 animals. Retained sutures were present in 10 of 12 animals.
Limitations: Animal experiment.
Conclusions: FTGB by using the SEMF technique and an endoscopic suturing device is technically feasible, reproducible, and safe. Larger tissue specimens will allow improved analysis of multiple cell types.
Copyright © 2012 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Figures



References
-
- Harberson J, Thomas RM, Harbison SP, Parkman HP. Gastric neuromuscular pathology in gastroparesis: analysis of full-thickness antral biopsies. Dig Dis Sci. 2010;55(2):359–70. - PubMed
-
- Horváth VJ, Vittal H, Lörincz A, Chen H, Almeida-Porada G, Redelman D, et al. Reduced stem cell factor links smooth myopathy and loss of interstitial cells of cajal in murine diabetic gastroparesis. Gastroenterology. 2006;130(3):759–70. - PubMed
-
- Farrugia G. Interstitial cells of Cajal in health and disease. Neurogastroenterol Motil. 2008;20 (Suppl 1):54–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
