

Cognitive reserve in ageing and Alzheimer's disease
- PMID: 23079557
- PMCID: PMC3507991
- DOI: 10.1016/S1474-4422(12)70191-6
Cognitive reserve in ageing and Alzheimer's disease
Abstract
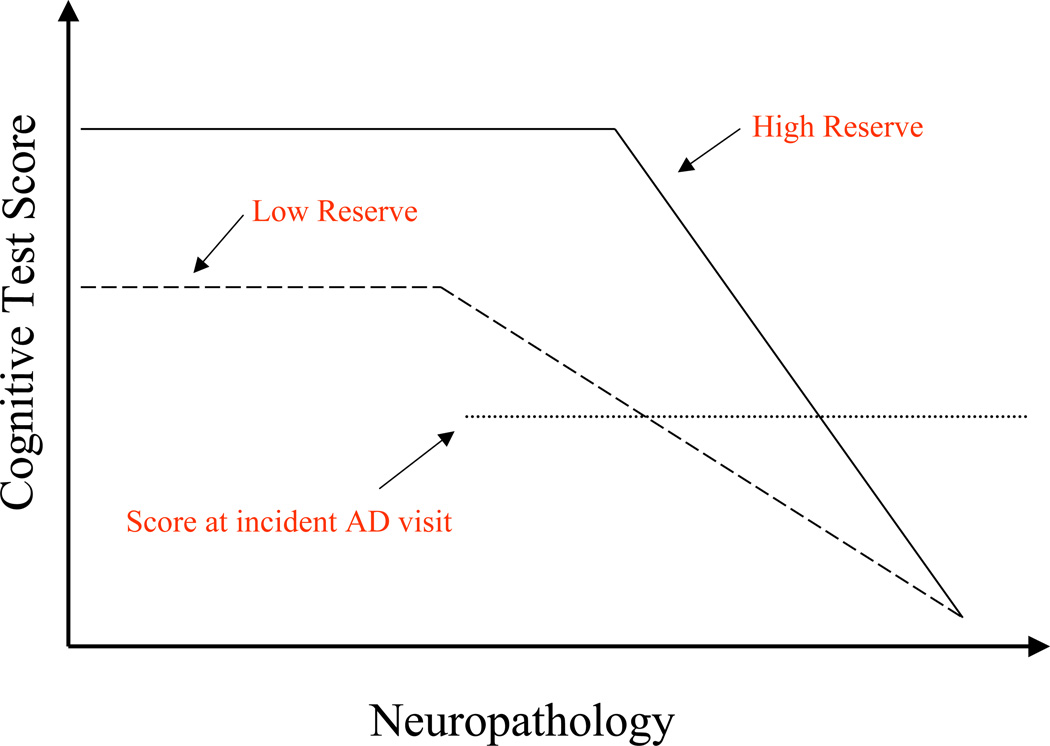
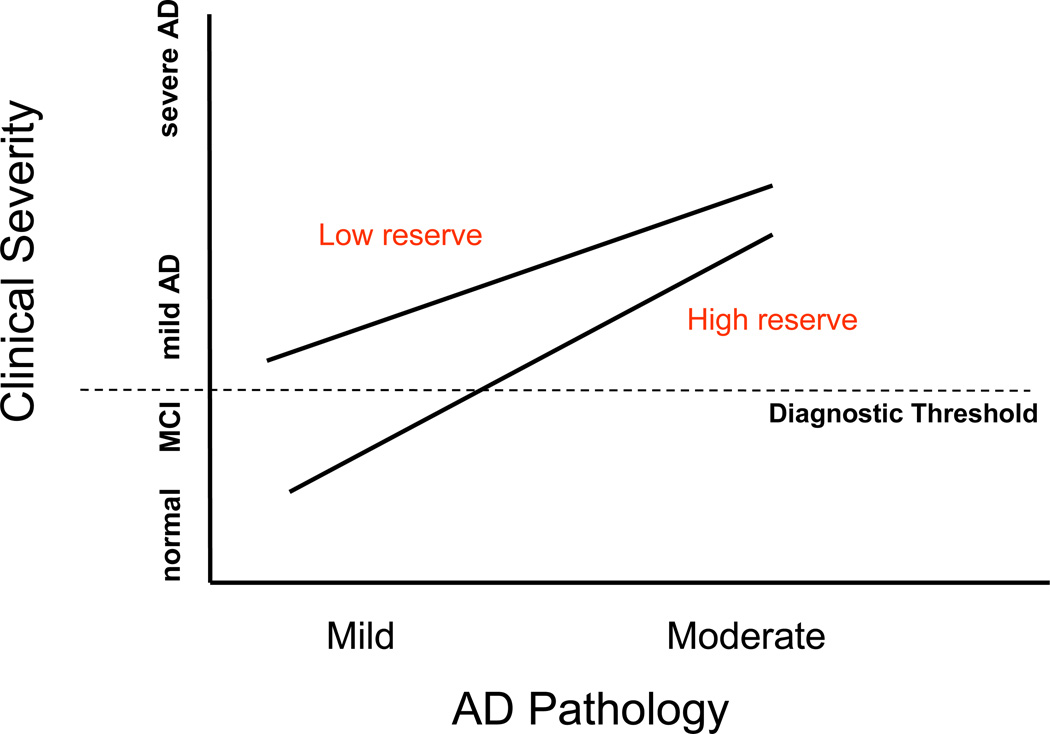
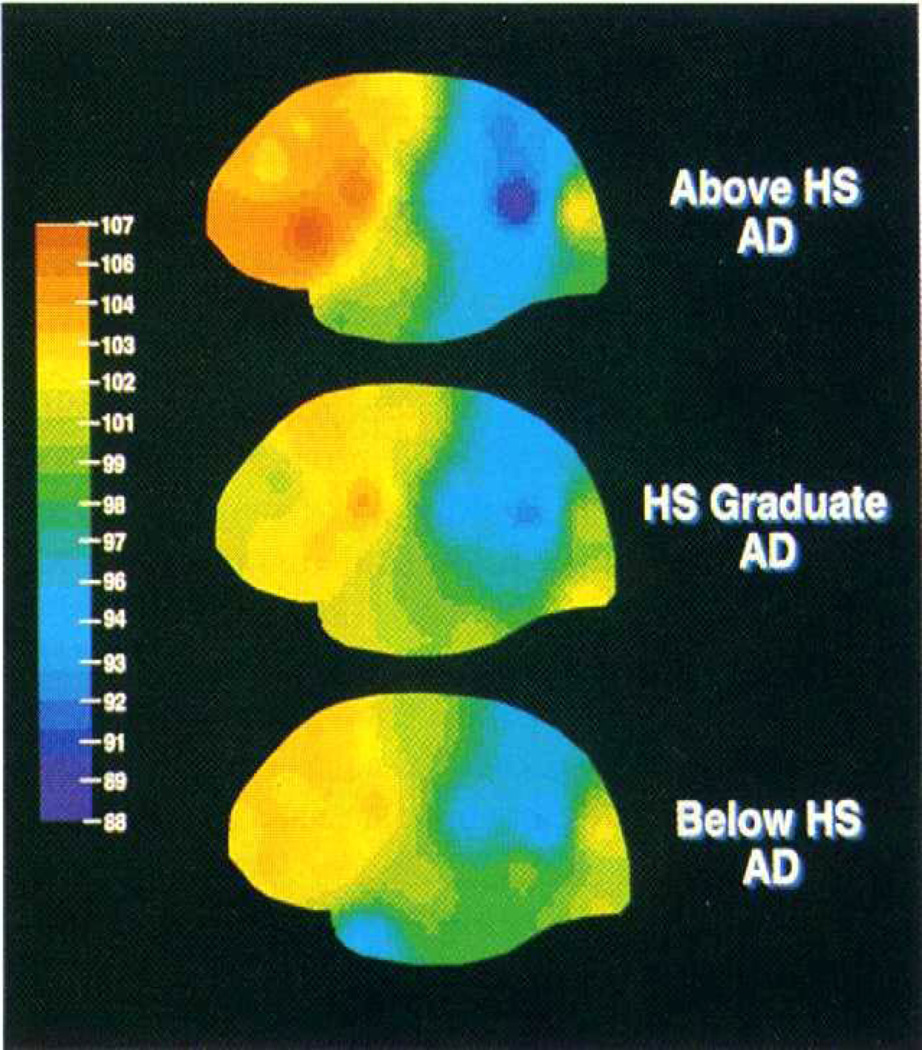
The concept of cognitive reserve provides an explanation for differences between individuals in susceptibility to age-related brain changes or pathology related to Alzheimer's disease, whereby some people can tolerate more of these changes than others and maintain function. Epidemiological studies suggest that lifelong experiences, including educational and occupational attainment, and leisure activities in later life, can increase this reserve. For example, the risk of developing Alzheimer's disease is reduced in individuals with higher educational or occupational attainment. Reserve can conveniently be divided into two types: brain reserve, which refers to differences in the brain structure that may increase tolerance to pathology, and cognitive reserve, which refers to differences between individuals in how tasks are performed that might enable some people to be more resilient to brain changes than others. Greater understanding of the concept of cognitive reserve could lead to interventions to slow cognitive ageing or reduce the risk of dementia.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Gurland B. The borderlands of dementia: the influence of sociocultural characteristics on rates of dementia occurring in the senium. Aging. 1981;15:61–84.
-
- Kittner SJ, White LR, Farmer ME, Wolz M, Kaplan E, Moes E, et al. Methodological issues in screening for dementia: The problem of education adjustment. Journal of Chronic Diseases. 1986;39:163–170. - PubMed
-
- Berkman LF. The association between educational attainment and mental status examinations: Of etiologic significance for senile dementias or not? Journal of Chronic Diseases. 1986;39:171–174. - PubMed
-
- Zhang M, Katzman R, Salmon D, Jin H, Cai G, Wang Z, et al. The prevalence of dementia and Alzheimer's disease in Shanghai, China: Impact of age, gender and education. Annals of Neurology. 1990;27:428–437. - PubMed
-
- Elkins JS, Longstreth WT, Manolio TA, Newman AB, Bhadelia RA, Johnston SC. Education and the cognitive decline associated with MRI-defined brain infarct. Neurology. 2006;67(3):435–440. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
