

Treatment of postmenopausal osteoporosis with delayed-release risedronate 35 mg weekly for 2 years
- PMID: 23079690
- PMCID: PMC3536960
- DOI: 10.1007/s00198-012-2175-7
Treatment of postmenopausal osteoporosis with delayed-release risedronate 35 mg weekly for 2 years
Abstract
Bone mineral density response to once weekly delayed-release formulation of risedronate, given before or following breakfast, was non-inferior to that seen with traditional immediate-release risedronate given daily before breakfast. Delayed-release risedronate is a convenient dosing regimen for oral bisphosphonate therapy that might avoid poor compliance.
Introduction: This 2-year, randomized, controlled, non-inferiority study assessed the efficacy and safety of a delayed-release (DR) 35-mg weekly oral formulation of risedronate that allows subjects to take their weekly risedronate dose before or immediately after breakfast. Results from the first year of the study were published previously (McClung et al. Osteoporos Int 23(1):267-276, 2012); we now report the final results after 2 years.
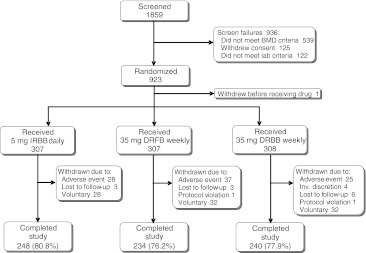
Methods: Women with postmenopausal osteoporosis were randomly assigned to receive risedronate 5 mg immediate-release (IR) daily (n = 307) at least 30 min before breakfast, or risedronate 35 mg DR weekly, either immediately following breakfast (FB, n = 307) or at least 30 min before breakfast (BB, n = 308). Bone mineral density (BMD), bone turnover markers (BTMs), fractures, adverse events, and bone histomorphometry were evaluated.
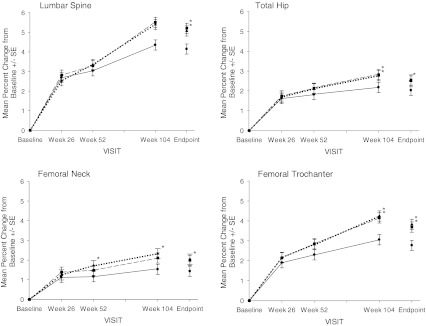
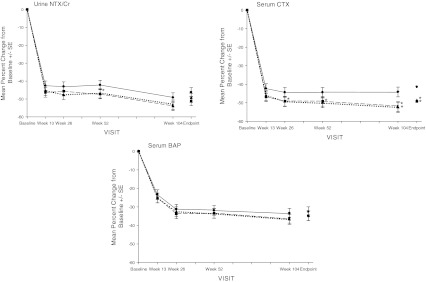
Results: A total of 248 subjects (80.8 %) in the IR daily group, 234 subjects (76.2 %) in the DR FB weekly group, and 240 subjects (77.9 %) in the DR BB weekly group completed the 2-year study. After 2 years of treatment, BMD increases at the lumbar spine and total hip with the weekly DR doses similar to or greater than that with the IR daily dose. Decreases in BTMs were similar or significantly lower in the DR groups. Bone histomorphometry results did not differ among the DR weekly and the IR daily formulations. The three regimens were similarly well tolerated.
Conclusions: Risedronate 35 mg DR weekly is as effective and as well tolerated as risedronate 5 mg IR daily, and will allow subjects to take their weekly risedronate dose immediately after breakfast.
Figures
References
-
- McClung MR, Miller PD, Brown J, Zanchetta J, Bolognese MA, Benhamou C-L, Balske A, Burgio D, Sarley J, Recker RR. Efficacy and safety of a novel delayed-release risedronate 35 mg once-a-week tablet in the treatment of postmenopausal osteoporosis. Osteoporos Int. 2012;23(1):267–276. doi: 10.1007/s00198-011-1791-y. - DOI - PMC - PubMed
-
- Ettinger B, Pressman A, Schein J, Chan J, Silver P, Connolly N. Alendronate use among 812 women: prevalence of gastrointestinal complaints, noncompliance with patient instructions, and discontinuation. J Manag Care Pharm. 1998;4(5):488–492.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
