

Twelve-year risk of revision after primary total hip replacement in the U.S. Medicare population
- PMID: 23079874
- PMCID: PMC3489069
- DOI: 10.2106/JBJS.K.00569
Twelve-year risk of revision after primary total hip replacement in the U.S. Medicare population
Abstract
Background: There is limited population-based literature on rates and risk factors for revision following primary total hip replacement.
Methods: We performed a retrospective cohort study of Medicare beneficiaries who had elective total hip replacement for osteoarthritis between July 1, 1995, and June 30, 1996. Patients were followed with use of Medicare claims through 2008. The primary end point was revision total hip replacement as indicated by hospital discharge codes according to the International Classification of Diseases, Ninth Revision. We used the Kaplan-Meier method to plot the risks of revision and of death over a twelve-year follow-up period. We used Cox proportional hazard regression models to identify preoperative risk factors for revision of primary total hip replacement. We conducted sensitivity analyses to account for competing risks of major comorbid conditions.
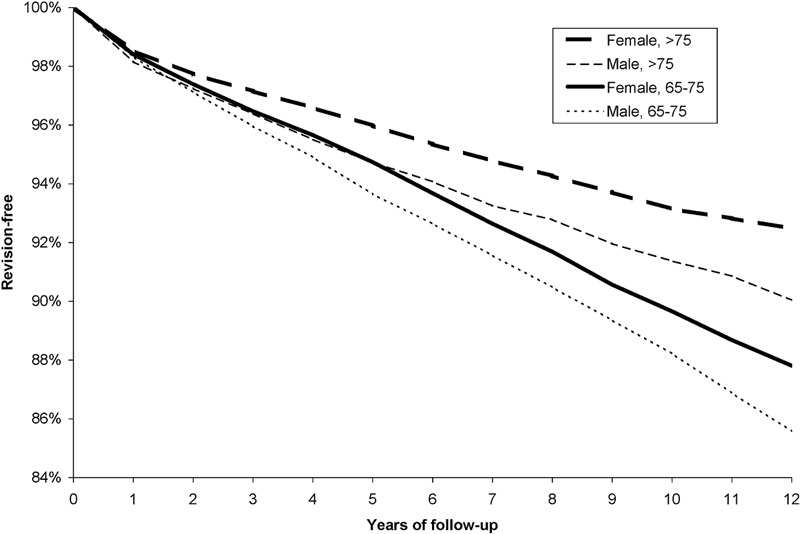
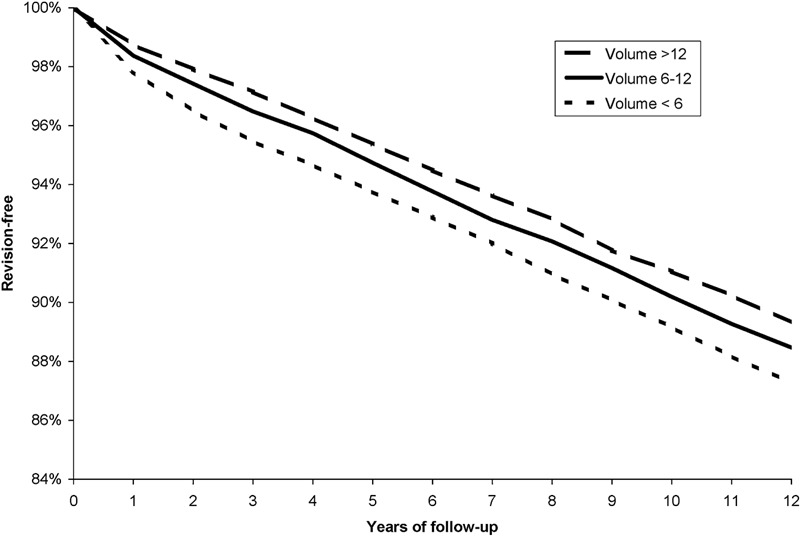
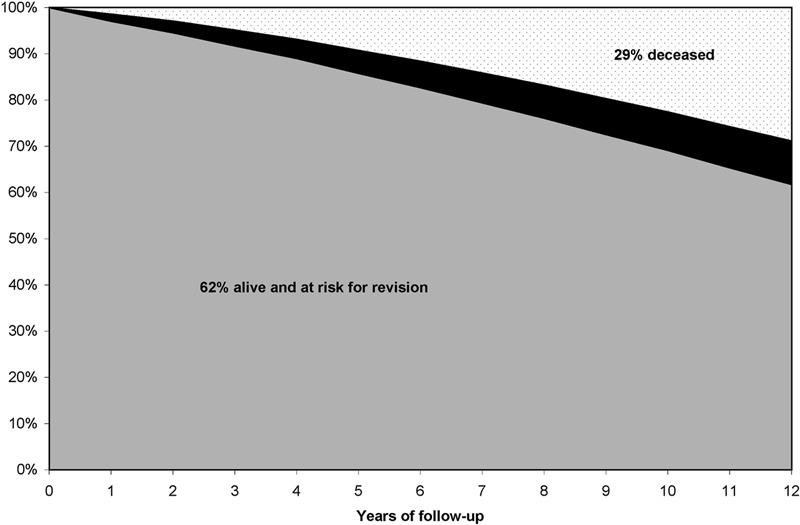
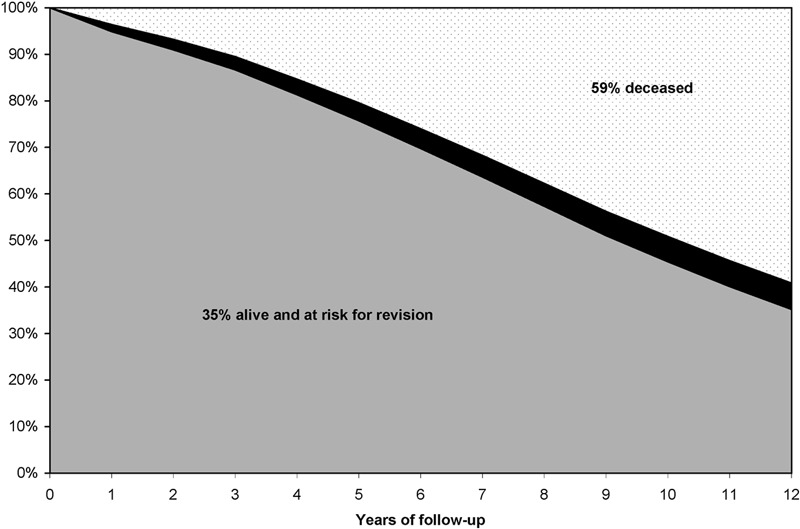
Results: The risk of revision total hip replacement for patients remaining alive was approximately 2% per year for the first eighteen months and then 1% per year for the remainder of the follow-up period. The absolute risk of death over the twelve-year follow-up period exceeded the risk of revision total hip replacement by a factor of ten (59% vs. 5.7%) in patients older than seventy-five years at the time of primary total hip replacement and by a factor of three (29% vs. 9.4%) in patients sixty-five to seventy-five years old at the time of surgery. In multivariate Cox proportional hazard models, the relative risk of revision was higher in men than in women (hazard ratio [HR], 1.23; 95% confidence interval [95% CI], 1.15, 1.31) and in patients sixty-five to seventy-five years of age at the time of primary total hip replacement than in those over seventy-five years (HR, 1.47; 95% CI, 1.37, 1.58). Patients of surgeons who performed fewer than six total hip replacements annually in the Medicare population had a higher risk of revision than those whose surgeons performed more than twelve per year (HR, 1.21; 95% CI, 1.12, 1.32).
Conclusions: Efforts to reduce the number of revision hip arthroplasties should be targeted at revisions occurring in the first eighteen months following the index arthroplasty, when revision risk is higher, and at younger patients, who are more likely to survive long enough to require revision. .
Figures
Comment in
-
Identifying strategies to improve patient outcomes in total hip replacement: commentary on an article by Jeffrey N. Katz, MD, MSc, et al.: ‘‘twelve-year risk of revision after primary total hip replacement in the U.S. Medicare population’’.J Bone Joint Surg Am. 2012 Oct 17;94(20):e153. doi: 10.2106/jbjs.l.00951. J Bone Joint Surg Am. 2012. PMID: 23243675 No abstract available.
References
-
- United States Department of Health & Human Services. HCUP nationwide inpatient sample. 2009.
-
- Hallan G, Lie SA, Furnes O, Engesaeter LB, Vollset SE, Havelin LI. Medium- and long-term performance of 11,516 uncemented primary femoral stems from the Norwegian arthroplasty register. J Bone Joint Surg Br. 2007;89:1574-80 - PubMed
-
- Mäkelä K, Eskelinen A, Pulkkinen P, Paavolainen P, Remes V. Cemented total hip replacement for primary osteoarthritis in patients aged 55 years or older: results of the 12 most common cemented implants followed for 25 years in the Finnish Arthroplasty Register. J Bone Joint Surg Br. 2008;90:1562-9 - PubMed
-
- Mäkelä KT, Eskelinen A, Pulkkinen P, Paavolainen P, Remes V. Total hip arthroplasty for primary osteoarthritis in patients fifty-five years of age or older. An analysis of the Finnish arthroplasty registry. J Bone Joint Surg Am. 2008;90:2160-70 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
