

Discrete choice experiment to evaluate factors that influence preferences for antibiotic prophylaxis in pediatric oncology
- PMID: 23082169
- PMCID: PMC3474806
- DOI: 10.1371/journal.pone.0047470
Discrete choice experiment to evaluate factors that influence preferences for antibiotic prophylaxis in pediatric oncology
Abstract
Background: Bacterial and fungal infections in pediatric oncology patients cause morbidity and mortality. The clinical utility of antimicrobial prophylaxis in children is uncertain and the personal utility of these agents is disputed. Objectives were to use a discrete choice experiment to: (1) describe the importance of attributes to parents and healthcare providers when deciding between use and non-use of antibacterial and antifungal prophylaxis; and (2) estimate willingness-to-pay for prophylactic strategies.
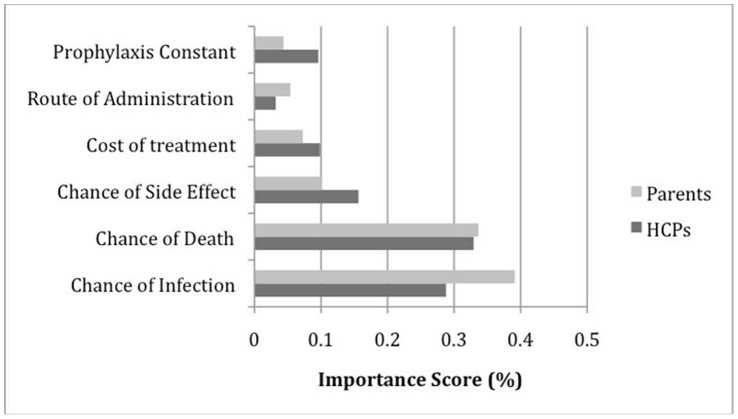
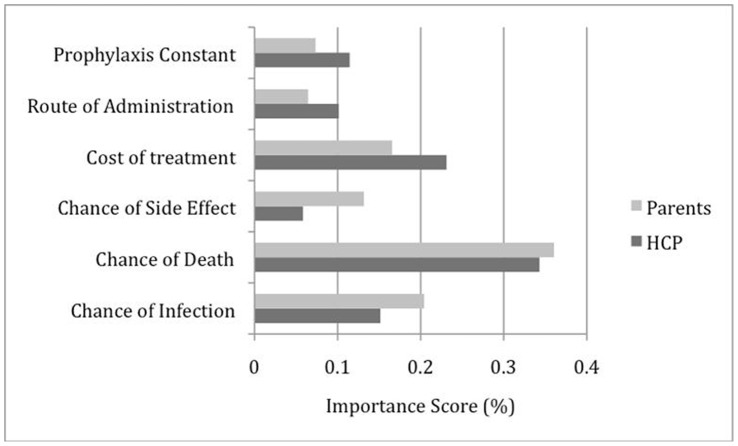
Methods: Attributes were chances of infection, death and side effects, route of administration and cost of pharmacotherapy. Respondents were randomized to a discrete choice experiment outlining hypothetical treatment options to prevent antibacterial or antifungal infections. Each respondent was presented 16 choice tasks and was asked to choose between two unlabeled treatment options and an opt-out alternative (no prophylaxis).
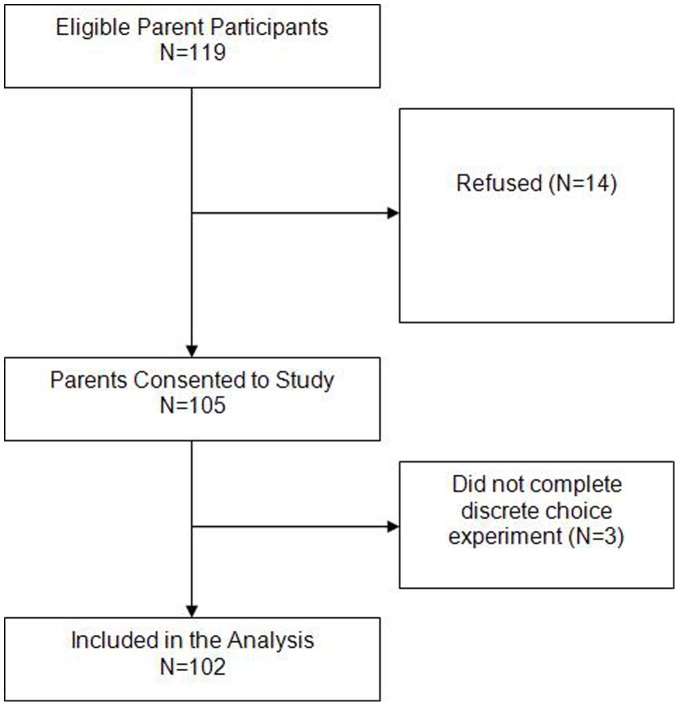
Results: 102 parents and 60 healthcare providers participated. For the antibacterial discrete choice experiment, frequency of administration was significantly associated with utility for parents but not for healthcare providers. Increasing chances of infection, death, side effects and cost were all significantly associated with decreased utility for parents and healthcare providers in both the antibacterial and antifungal discrete choice experiment. Parental willingness-to-pay was higher than healthcare providers for both strategies.
Conclusion: Chances of infection, death, side effects and costs were all significantly associated with utility. Parents have higher willingness-to-pay for these strategies compared with healthcare providers. This knowledge can help to develop prophylaxis programs.
Conflict of interest statement
Figures
References
-
- Sung L, Lange BJ, Gerbing RB, Alonzo TA, Feusner J (2007) Microbiologically documented infections and infection-related mortality in children with acute myeloid leukemia. Blood 110: 3532–3539. - PubMed
-
- Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH (2006) Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 106: 2258–2266. - PubMed
-
- Gafter-Gvili A, Fraser A, Paul M, Leibovici L (2005) Meta-analysis: antibiotic prophylaxis reduces mortality in neutropenic patients. Ann Intern Med 142: 979–995. - PubMed
-
- Robenshtok E, Gafter-Gvili A, Goldberg E, Weinberger M, Yeshurun M, et al. (2007) Antifungal prophylaxis in cancer patients after chemotherapy or hematopoietic stem-cell transplantation: systematic review and meta-analysis. J Clin Oncol 25(34): 5471–5489. - PubMed
-
- Lehrnbecher L, Ethier MC, Zaoutis T, Creutzig U, Gamis A, et al. (2009) International variations in infection supportive care practices for paediatric patients with acute myeloid leukaemia. Br J Haematol 147: 125–128. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
