

A flexible alternative to the Cox proportional hazards model for assessing the prognostic accuracy of hospice patient survival
- PMID: 23082220
- PMCID: PMC3474724
- DOI: 10.1371/journal.pone.0047804
A flexible alternative to the Cox proportional hazards model for assessing the prognostic accuracy of hospice patient survival
Abstract
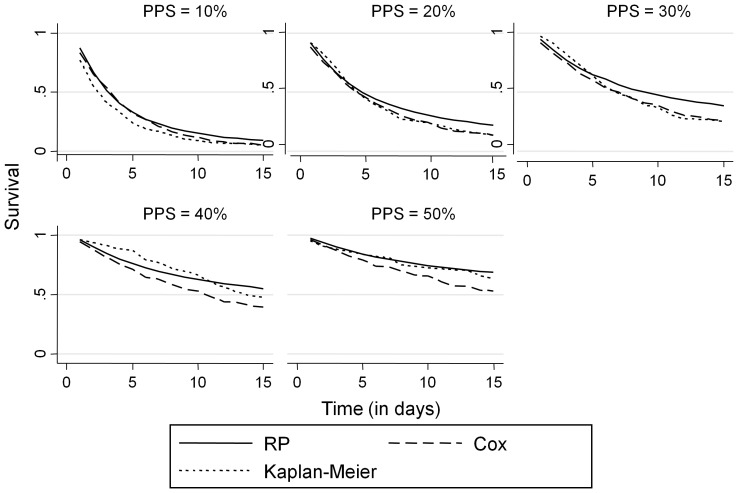
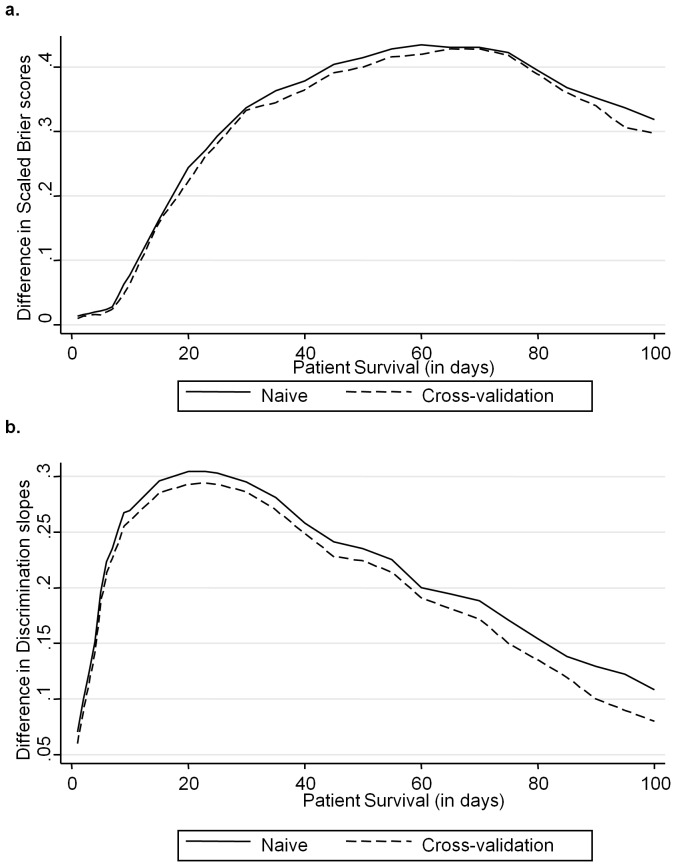
Prognostic models are often used to estimate the length of patient survival. The Cox proportional hazards model has traditionally been applied to assess the accuracy of prognostic models. However, it may be suboptimal due to the inflexibility to model the baseline survival function and when the proportional hazards assumption is violated. The aim of this study was to use internal validation to compare the predictive power of a flexible Royston-Parmar family of survival functions with the Cox proportional hazards model. We applied the Palliative Performance Scale on a dataset of 590 hospice patients at the time of hospice admission. The retrospective data were obtained from the Lifepath Hospice and Palliative Care center in Hillsborough County, Florida, USA. The criteria used to evaluate and compare the models' predictive performance were the explained variation statistic R(2), scaled Brier score, and the discrimination slope. The explained variation statistic demonstrated that overall the Royston-Parmar family of survival functions provided a better fit (R(2) =0.298; 95% CI: 0.236-0.358) than the Cox model (R(2) =0.156; 95% CI: 0.111-0.203). The scaled Brier scores and discrimination slopes were consistently higher under the Royston-Parmar model. Researchers involved in prognosticating patient survival are encouraged to consider the Royston-Parmar model as an alternative to Cox.
Conflict of interest statement
Figures




Similar articles
-
The current application of the Royston-Parmar model for prognostic modeling in health research: a scoping review.Diagn Progn Res. 2018 Feb 7;2:4. doi: 10.1186/s41512-018-0026-5. eCollection 2018. Diagn Progn Res. 2018. PMID: 31093554 Free PMC article.
-
External validation of a web-based prognostic tool for predicting survival for patients in hospice care.J Palliat Care. 2013 Autumn;29(3):140-6. J Palliat Care. 2013. PMID: 24380212
-
Survival analysis of irish amyotrophic lateral sclerosis patients diagnosed from 1995-2010.PLoS One. 2013 Sep 30;8(9):e74733. doi: 10.1371/journal.pone.0074733. eCollection 2013. PLoS One. 2013. PMID: 24098664 Free PMC article.
-
Construction and validation of a prognostic model across several studies, with an application in superficial bladder cancer.Stat Med. 2004 Mar 30;23(6):907-26. doi: 10.1002/sim.1691. Stat Med. 2004. PMID: 15027080
-
Predicting survival with the Palliative Performance Scale in a minority-serving hospice and palliative care program.J Pain Symptom Manage. 2009 Apr;37(4):642-8. doi: 10.1016/j.jpainsymman.2008.03.023. Epub 2008 Sep 26. J Pain Symptom Manage. 2009. PMID: 18823751 Free PMC article.
Cited by
-
Performance evaluation of survival regression models in analysing Swedish dental implant complication data with frailty.PLoS One. 2021 Jan 7;16(1):e0245111. doi: 10.1371/journal.pone.0245111. eCollection 2021. PLoS One. 2021. PMID: 33411801 Free PMC article. Clinical Trial.
-
Natural disease progression and novel survival prediction model for hepatocellular carcinoma with spinal metastases: a 10-year single-center study.World J Surg Oncol. 2020 Jun 20;18(1):135. doi: 10.1186/s12957-020-01913-9. World J Surg Oncol. 2020. PMID: 32563268 Free PMC article. Clinical Trial.
-
Examining the effects of social assistance on suicide-related behaviour among impoverished older adults in Korea using a nationwide cohort study from 2010-2019.Sci Rep. 2024 Jul 18;14(1):16632. doi: 10.1038/s41598-024-61845-2. Sci Rep. 2024. PMID: 39025874 Free PMC article.
-
Recurrent emergent hernia repairs: who is at risk?Surg Endosc. 2025 Jul;39(7):4599-4607. doi: 10.1007/s00464-025-11914-y. Epub 2025 Jun 19. Surg Endosc. 2025. PMID: 40537684 Free PMC article.
-
The current application of the Royston-Parmar model for prognostic modeling in health research: a scoping review.Diagn Progn Res. 2018 Feb 7;2:4. doi: 10.1186/s41512-018-0026-5. eCollection 2018. Diagn Progn Res. 2018. PMID: 31093554 Free PMC article.
References
-
- Royston P, Moons KG, Altman DG, Vergouwe Y (2009) Prognosis and prognostic research: Developing a prognostic model. BMJ 338: b604. - PubMed
-
- Vickers AJ (2011) Prediction models: revolutionary in principle, but do they do more good than harm? J Clin Oncol 29: 2951–2952. - PubMed
-
- Moons KG, Altman DG, Vergouwe Y, Royston P (2009) Prognosis and prognostic research: application and impact of prognostic models in clinical practice. BMJ 338: b606. - PubMed
-
- Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, et al. (2000) Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 284: 2476–2482. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
