

Optimal glycemic control in neurocritical care patients: a systematic review and meta-analysis
- PMID: 23082798
- PMCID: PMC3682305
- DOI: 10.1186/cc11812
Optimal glycemic control in neurocritical care patients: a systematic review and meta-analysis
Abstract
Introduction: Hyper- and hypoglycemia are strongly associated with adverse outcomes in critical care. Neurologically injured patients are a unique subgroup, where optimal glycemic targets may differ, such that the findings of clinical trials involving heterogeneous critically ill patients may not apply.
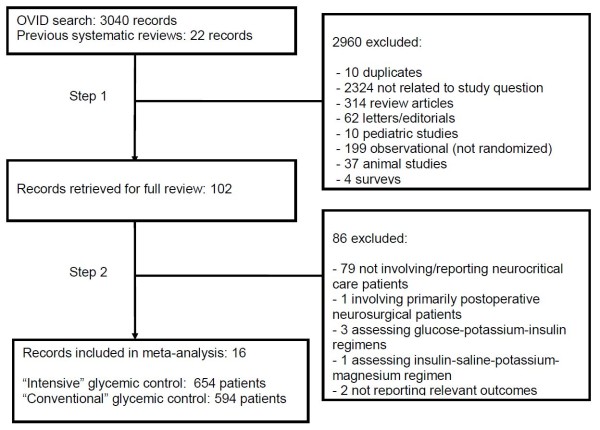
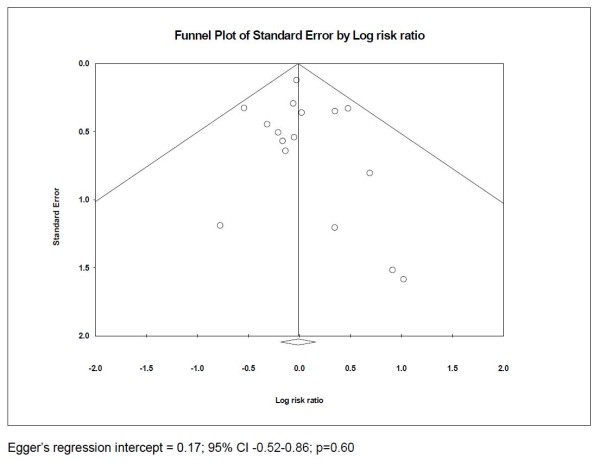
Methods: We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing intensive insulin therapy with conventional glycemic control among patients with traumatic brain injury, ischemic or hemorrhagic stroke, anoxic encephalopathy, central nervous system infections or spinal cord injury.
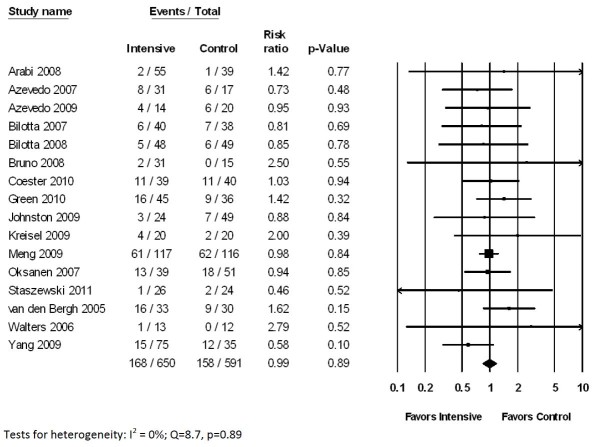
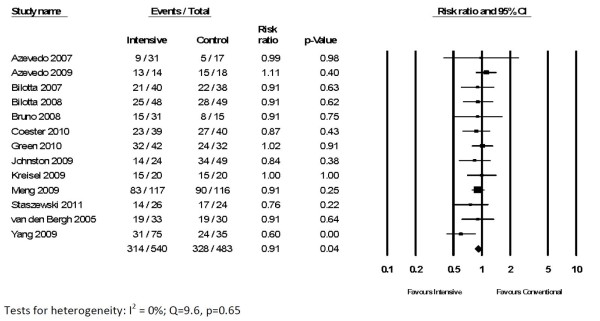
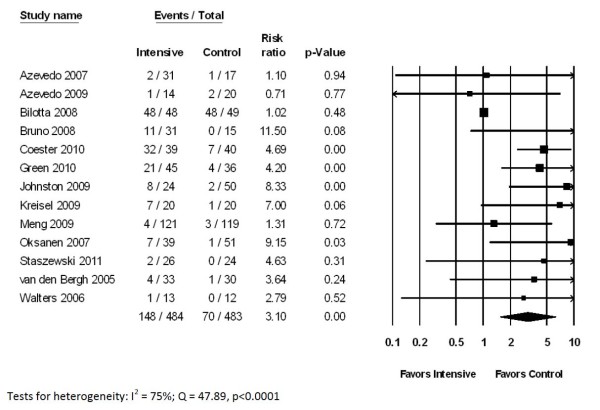
Results: Sixteen RCTs, involving 1248 neurocritical care patients, were included. Glycemic targets with intensive insulin ranged from 70-140 mg/dl (3.9-7.8 mmol/L), while conventional protocols aimed to keep glucose levels below 144-300 mg/dl (8.0-16.7 mmol/L). Tight glycemic control had no impact on mortality (RR 0.99; 95% CI 0.83-1.17; p = 0.88), but did result in fewer unfavorable neurological outcomes (RR 0.91; 95% CI 0.84-1.00; p = 0.04). However, improved outcomes were only observed when glucose levels in the conventional glycemic control group were permitted to be relatively high [threshold for insulin administration > 200 mg/dl (> 11.1 mmol/L)], but not with more intermediate glycemic targets [threshold for insulin administration 140-180 mg/dl (7.8-10.0 mmol/L)]. Hypoglycemia was far more common with intensive therapy (RR 3.10; 95% CI 1.54-6.23; p = 0.002), but there was a large degree of heterogeneity in the results of individual trials (Q = 47.9; p<0.0001; I2 = 75%). Mortality was non-significantly higher with intensive insulin in studies where the proportion of patients developing hypoglycemia was large (> 33%) (RR 1.17; 95% CI 0.79-1.75; p = 0.44).
Conclusions: Intensive insulin therapy significantly increases the risk of hypoglycemia and does not influence mortality among neurocritical care patients. Very loose glucose control is associated with worse neurological recovery and should be avoided. These results suggest that intermediate glycemic goals may be most appropriate.
Figures
Comment in
-
Optimal glycemic control in neurocritical care patients.Crit Care. 2012 Oct 30;16(5):163. doi: 10.1186/cc11521. Crit Care. 2012. PMID: 23106972 Free PMC article.
Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Glycemic control, mortality, and hypoglycemia in critically ill patients: a systematic review and network meta-analysis of randomized controlled trials.Intensive Care Med. 2017 Jan;43(1):1-15. doi: 10.1007/s00134-016-4523-0. Epub 2016 Sep 16. Intensive Care Med. 2017. PMID: 27637719
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Oral anti-diabetic agents for women with established diabetes/impaired glucose tolerance or previous gestational diabetes planning pregnancy, or pregnant women with pre-existing diabetes.Cochrane Database Syst Rev. 2017 Oct 18;10(10):CD007724. doi: 10.1002/14651858.CD007724.pub3. Cochrane Database Syst Rev. 2017. PMID: 29045765 Free PMC article.
-
Insulin and oral agents for managing cystic fibrosis-related diabetes.Cochrane Database Syst Rev. 2016 Apr 18;4:CD004730. doi: 10.1002/14651858.CD004730.pub4. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2020 Oct 19;10:CD004730. doi: 10.1002/14651858.CD004730.pub5. PMID: 27087121 Updated.
Cited by
-
Blood glucose control using a computer-guided glucose management system in allogeneic hematopoietic cell transplant recipients.Bone Marrow Transplant. 2016 Jul;51(7):973-9. doi: 10.1038/bmt.2016.78. Epub 2016 Apr 4. Bone Marrow Transplant. 2016. PMID: 27042836
-
Expert consensus on the glycemic management of critically ill patients.J Intensive Med. 2022 Jul 8;2(3):131-145. doi: 10.1016/j.jointm.2022.06.001. eCollection 2022 Jul. J Intensive Med. 2022. PMID: 36789019 Free PMC article. No abstract available.
-
Continuous glucose monitoring in the ICU: clinical considerations and consensus.Crit Care. 2017 Jul 31;21(1):197. doi: 10.1186/s13054-017-1784-0. Crit Care. 2017. PMID: 28756769 Free PMC article. Review.
-
Stress-Induced Hyperglycemia Predicts Poor Outcomes in Primary Intracerebral Hemorrhage Patients.NeuroSci. 2025 Feb 2;6(1):12. doi: 10.3390/neurosci6010012. NeuroSci. 2025. PMID: 39982264 Free PMC article.
-
Intensive versus conventional glucose control in critically ill patients with traumatic brain injury: long-term follow-up of a subgroup of patients from the NICE-SUGAR study.Intensive Care Med. 2015 Jun;41(6):1037-47. doi: 10.1007/s00134-015-3757-6. Epub 2015 Jun 19. Intensive Care Med. 2015. PMID: 26088909 Clinical Trial.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
