

Clinical pharmacology of analgesics assessed with human experimental pain models: bridging basic and clinical research
- PMID: 23082949
- PMCID: PMC3579278
- DOI: 10.1111/bph.12023
Clinical pharmacology of analgesics assessed with human experimental pain models: bridging basic and clinical research
Abstract
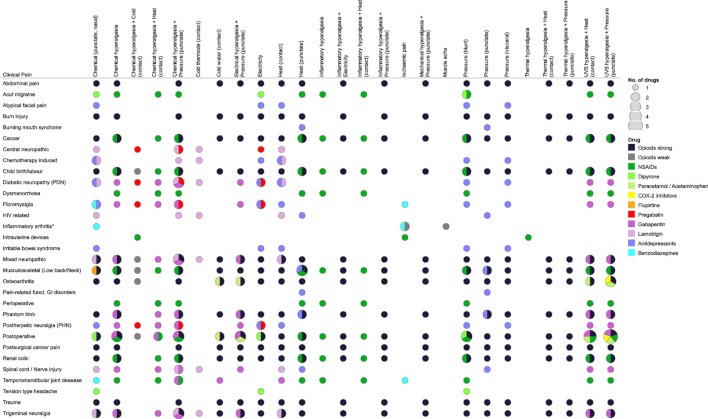
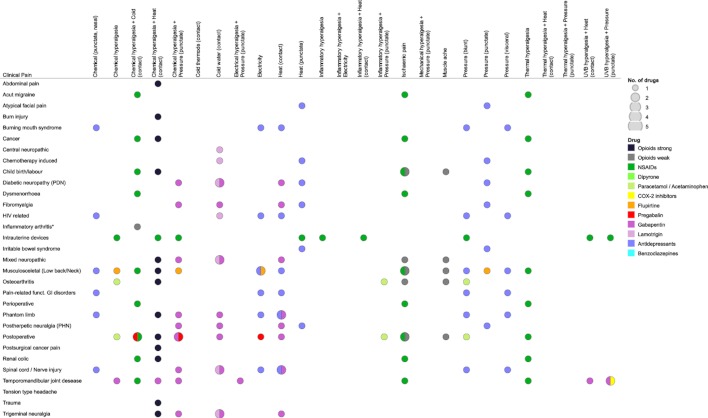
The medical impact of pain is such that much effort is being applied to develop novel analgesic drugs directed towards new targets and to investigate the analgesic efficacy of known drugs. Ongoing research requires cost-saving tools to translate basic science knowledge into clinically effective analgesic compounds. In this review we have re-examined the prediction of clinical analgesia by human experimental pain models as a basis for model selection in phase I studies. The overall prediction of analgesic efficacy or failure of a drug correlated well between experimental and clinical settings. However, correct model selection requires more detailed information about which model predicts a particular clinical pain condition. We hypothesized that if an analgesic drug was effective in an experimental pain model and also a specific clinical pain condition, then that model might be predictive for that particular condition and should be selected for development as an analgesic for that condition. The validity of the prediction increases with an increase in the numbers of analgesic drug classes for which this agreement was shown. From available evidence, only five clinical pain conditions were correctly predicted by seven different pain models for at least three different drugs. Most of these models combine a sensitization method. The analysis also identified several models with low impact with respect to their clinical translation. Thus, the presently identified agreements and non-agreements between analgesic effects on experimental and on clinical pain may serve as a solid basis to identify complex sets of human pain models that bridge basic science with clinical pain research.
© 2012 The Authors. British Journal of Pharmacology © 2012 The British Pharmacological Society.
Figures

Similar articles
-
Human models of pain for the prediction of clinical analgesia.Pain. 2014 Oct;155(10):2014-21. doi: 10.1016/j.pain.2014.07.003. Epub 2014 Jul 11. Pain. 2014. PMID: 25020003
-
Role of neuroimaging in analgesic drug development.Drugs R D. 2008;9(5):323-34. doi: 10.2165/00126839-200809050-00003. Drugs R D. 2008. PMID: 18721001 Free PMC article. Review.
-
Current evidence of cannabinoid-based analgesia obtained in preclinical and human experimental settings.Eur J Pain. 2018 Mar;22(3):471-484. doi: 10.1002/ejp.1148. Epub 2017 Nov 21. Eur J Pain. 2018. PMID: 29160600 Review.
-
Use of analgesic drugs for pain management in sheep.N Z Vet J. 2012 Mar;60(2):87-94. doi: 10.1080/00480169.2011.642772. N Z Vet J. 2012. PMID: 22352925 Review.
-
Basic pharmacology and advances in emergency medicine.Emerg Med Clin North Am. 2005 May;23(2):433-65, ix-x. doi: 10.1016/j.emc.2004.12.010. Emerg Med Clin North Am. 2005. PMID: 15829391 Review.
Cited by
-
Pain, Smell, and Taste in Adults: A Narrative Review of Multisensory Perception and Interaction.Pain Ther. 2021 Jun;10(1):245-268. doi: 10.1007/s40122-021-00247-y. Epub 2021 Feb 26. Pain Ther. 2021. PMID: 33635507 Free PMC article. Review.
-
12/15-lipoxygenases mediate toll-like receptor 4-dependent nociplastic pain hypersensitivity in female mice.Pain. 2025 Jul 10:10.1097/j.pain.0000000000003711. doi: 10.1097/j.pain.0000000000003711. Online ahead of print. Pain. 2025. PMID: 40667997
-
Na+-dependent inactivation of vascular Na+/Ca2+ exchanger responsible for reduced peripheral blood flow in neuropathic pain model.Eur J Pharmacol. 2021 Nov 5;910:174448. doi: 10.1016/j.ejphar.2021.174448. Epub 2021 Aug 26. Eur J Pharmacol. 2021. PMID: 34454926 Free PMC article.
-
Lost but making progress--Where will new analgesic drugs come from?Sci Transl Med. 2014 Aug 13;6(249):249sr3. doi: 10.1126/scitranslmed.3008320. Sci Transl Med. 2014. PMID: 25122640 Free PMC article. Review.
-
Molecular signatures of mouse TRPV1-lineage neurons revealed by RNA-Seq transcriptome analysis.J Pain. 2014 Dec;15(12):1338-1359. doi: 10.1016/j.jpain.2014.09.010. Epub 2014 Oct 2. J Pain. 2014. PMID: 25281809 Free PMC article.
References
-
- Ahmad G, O'Flynn H, Attarbashi S, Duffy JM, Watson A. Pain relief for outpatient hysteroscopy. Cochrane Database Syst Rev. 2010;(11) CD007710. - PubMed
-
- Allen C, Hopewell S, Prentice A, Gregory D. Nonsteroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst Rev. 2009a;(2) CD004753. - PubMed
-
- Allen RH, Bartz D, Grimes DA, Hubacher D, O'Brien P. Interventions for pain with intrauterine device insertion. Cochrane Database Syst Rev. 2009b;(3) CD007373. - PubMed
-
- Alstergren P, Ernberg M, Nilsson M, Hajati AK, Sessle BJ, Kopp S. Glutamate-induced temporomandibular joint pain in healthy individuals is partially mediated by peripheral NMDA receptors. J Orofac Pain. 2010;24:172–180. - PubMed
-
- Altis K, Schmidtko A, Angioni C, Kuczka K, Schmidt H, Geisslinger G, et al. Analgesic efficacy of tramadol, pregabalin and ibuprofen in menthol-evoked cold hyperalgesia. Pain. 2009;147:116–121. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
