

Quality of diabetes mellitus care by rural primary care physicians
- PMID: 23083082
- PMCID: PMC3481192
- DOI: 10.1111/j.1748-0361.2012.00410.x
Quality of diabetes mellitus care by rural primary care physicians
Abstract
Purpose: To explore the relationship between degree of rurality and glucose (hemoglobin A1c), blood pressure (BP), and lipid (LDL) control among patients with diabetes.
Methods: Descriptive study; 1,649 patients in 205 rural practices in the United States. Patients' residence ZIP codes defined degree of rurality (Rural-Urban Commuting Areas codes). Outcomes were measures of acceptable control (A1c < = 9%, BP < 140/90 mmHg, LDL < 130 mg/dL) and optimal control (A1c < 7%, BP < 130/80 mmHg, LDL < 100 mg/dL). Statistical significance was set at P < .008 (Bonferroni's correction).
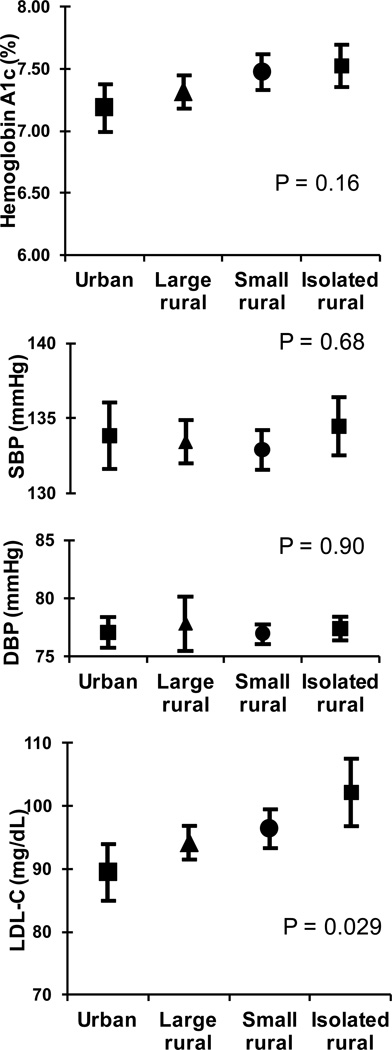
Findings: Although the proportion of patients with reasonable A1c control worsened by increasing degree of rurality, the differences were not statistically significant (urban 90%, large rural 88%, small rural 85%, isolated rural 83%; P = .10); mean A1c values also increased by degree of rurality, although not statistically significant (urban 7.2 [SD 1.6], large rural 7.3 [SD 1.7], small rural 7.5 [SD 1.8], isolated rural 7.5 [SD 1.9]; P = .16). We observed no differences between degree of rural and reasonable BP or LDL control (P = .42, P = .23, respectively) or optimal A1c or BP control (P = .52, P = .65, respectively). Optimal and mean LDL values worsened as rurality increased (P = .08, P = .029, respectively).
Conclusions: In patients with diabetes who seek care in the rural Southern United States, we observed no relationship between degree of rurality of patients' residence and traditional measures of quality of care. Further examination of the trends and explanatory factors for relative worsening of metabolic control by increasing degree of rurality is warranted.
© 2012 National Rural Health Association.
Figures

References
-
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2008.
-
- Centers for Disease Control and Prevention. [Accessed December 22, 2011];Diabetes Public Health Resource. Available at: http://www.cdc.gov/diabetes/statistics/index.htm.
-
- Utz S. Diabetes care among rural Americans. Annu Rev Nurs Res. 2008;26:3–39. - PubMed
-
- Krishna S, Gillespie K, McBride T. Diabetes burden and access to preventive care in the rural United States. J Rural Health. 2010;26(1):3–11. - PubMed
-
- Andrus M, Kelley K, Murphey L, Herndon K. A comparison of diabetes care in rural and urban medical clinics in Alabama. J Community Health. 2004;29(1):29–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
