

Not all beta-blockers are equal in the management of long QT syndrome types 1 and 2: higher recurrence of events under metoprolol
- PMID: 23083782
- PMCID: PMC3515779
- DOI: 10.1016/j.jacc.2012.07.046
Not all beta-blockers are equal in the management of long QT syndrome types 1 and 2: higher recurrence of events under metoprolol
Abstract
Objectives: The purpose of this study was to compare the efficacy of beta-blockers in congenital long QT syndrome (LQTS).
Background: Beta-blockers are the mainstay in managing LQTS. Studies comparing the efficacy of commonly used beta-blockers are lacking, and clinicians generally assume they are equally effective.
Methods: Electrocardiographic and clinical parameters of 382 LQT1/LQT2 patients initiated on propranolol (n = 134), metoprolol (n = 147), and nadolol (n = 101) were analyzed, excluding patients <1 year of age at beta-blocker initiation. Symptoms before therapy and the first breakthrough cardiac events (BCEs) were documented.
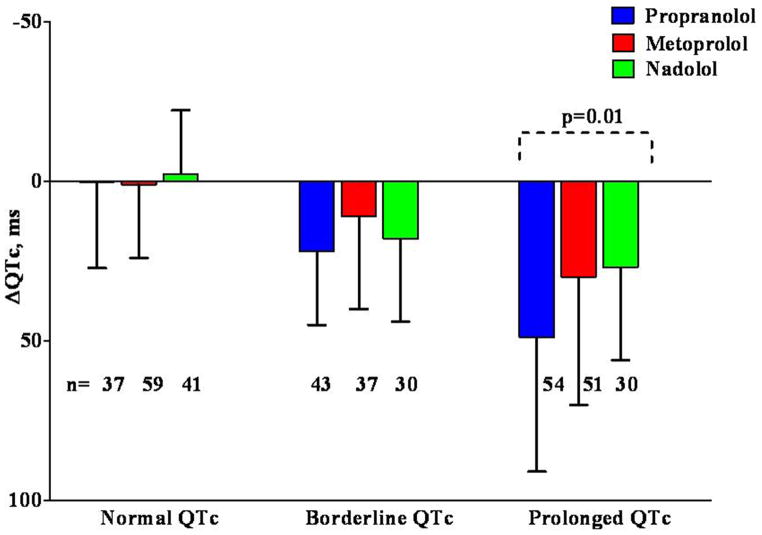
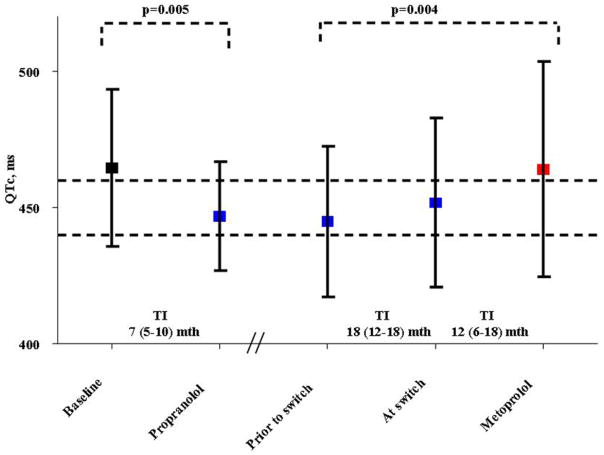
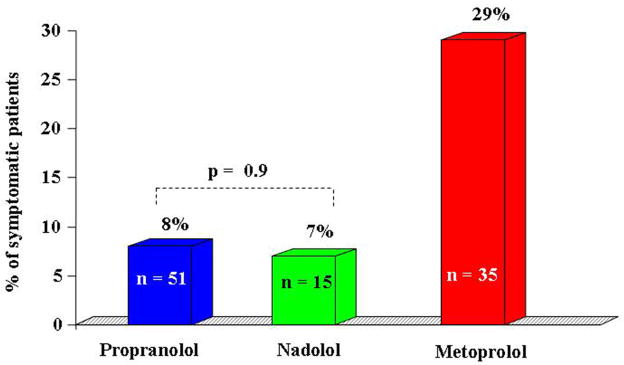
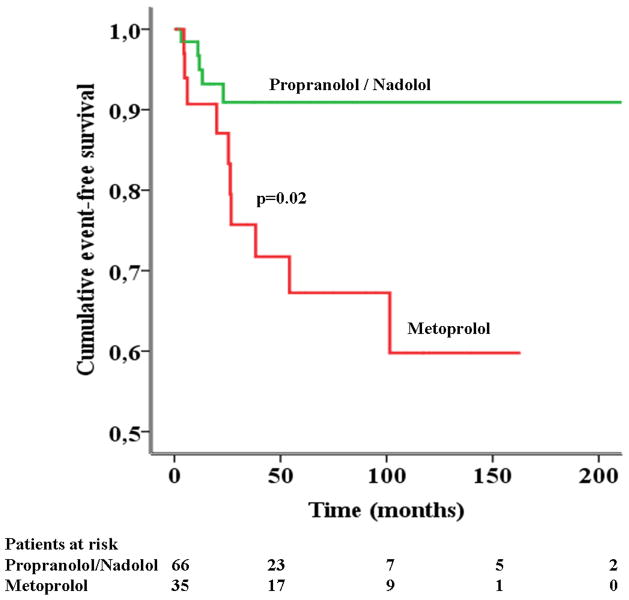
Results: Patients (56% female, 27% symptomatic, heart rate 76 ± 16 beats/min, QTc 472 ± 46 ms) were started on beta-blocker therapy at a median age of 14 years (interquartile range: 8 to 32 years). The QTc shortening with propranolol was significantly greater than with other beta-blockers in the total cohort and in the subset with QTc >480 ms. None of the asymptomatic patients had BCEs. Among symptomatic patients (n = 101), 15 had BCEs (all syncopes). The QTc shortening was significantly less pronounced among patients with BCEs. There was a greater risk of BCEs for symptomatic patients initiated on metoprolol compared to users of the other 2 beta-blockers combined, after adjustment for genotype (odds ratio: 3.95, 95% confidence interval: 1.2 to 13.1, p = 0.025). Kaplan-Meier analysis showed a significantly lower event-free survival for symptomatic patients receiving metoprolol compared to propranolol/nadolol.
Conclusions: Propranolol has a significantly better QTc shortening effect compared to metoprolol and nadolol, especially in patients with prolonged QTc. Propranolol and nadolol are equally effective, whereas symptomatic patients started on metoprolol are at a significantly higher risk for BCEs. Metoprolol should not be used for symptomatic LQT1 and LQT2 patients.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Novel insights into beta-blocker therapy for long QT syndromes.J Am Coll Cardiol. 2012 Nov 13;60(20):2100-2. doi: 10.1016/j.jacc.2012.08.965. Epub 2012 Oct 17. J Am Coll Cardiol. 2012. PMID: 23083777 No abstract available.
References
-
- Schwartz PJ, Periti M, Malliani A. The long Q-T syndrome. Am Heart J. 1975;89:378–90. - PubMed
-
- Schwartz PJ. Idiopathic long QT syndrome: Progress and Questions. Am Heart J. 1985;109:399–411. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Effectiveness and limitations of beta-blocker therapy in congenital long-QT syndrome. Circulation. 2000;101:616–23. - PubMed
-
- Shimizu W, Tanabe Y, Aiba T, et al. Differential effects of beta-blockade on dispersion of repolarization in the absence and presence of sympathetic stimulation between the LQT1 and LQT2 forms of congenital long QT syndrome. J Am Coll Cardiol. 2002;39:1984–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
