

David valve-sparing aortic root replacement: equivalent mid-term outcome for different valve types with or without connective tissue disorder
- PMID: 23083792
- PMCID: PMC6382393
- DOI: 10.1016/j.jtcvs.2012.09.013
David valve-sparing aortic root replacement: equivalent mid-term outcome for different valve types with or without connective tissue disorder
Abstract
Objective: Although implicitly accepted by many that the durability of valve-sparing aortic root replacement in patients with bicuspid aortic valve disease and connective tissue disorders will be inferior, this hypothesis has not been rigorously investigated.
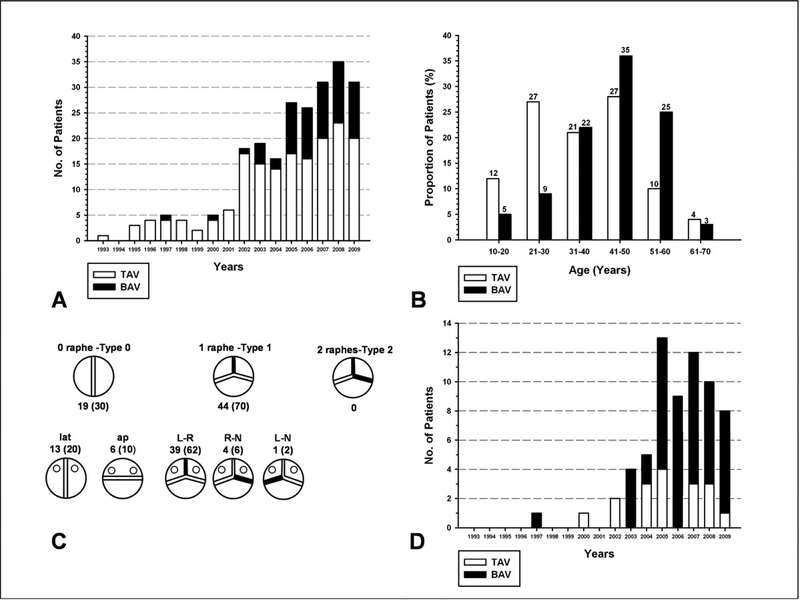
Methods: From 1993 to 2009, 233 patients (27% bicuspid aortic valve, 40% Marfan syndrome) underwent Tirone David valve-sparing aortic root replacement. Follow-up averaged 4.7 ± 3.3 years (1102 patient-years). Freedom from adverse outcomes was determined using log-rank calculations.
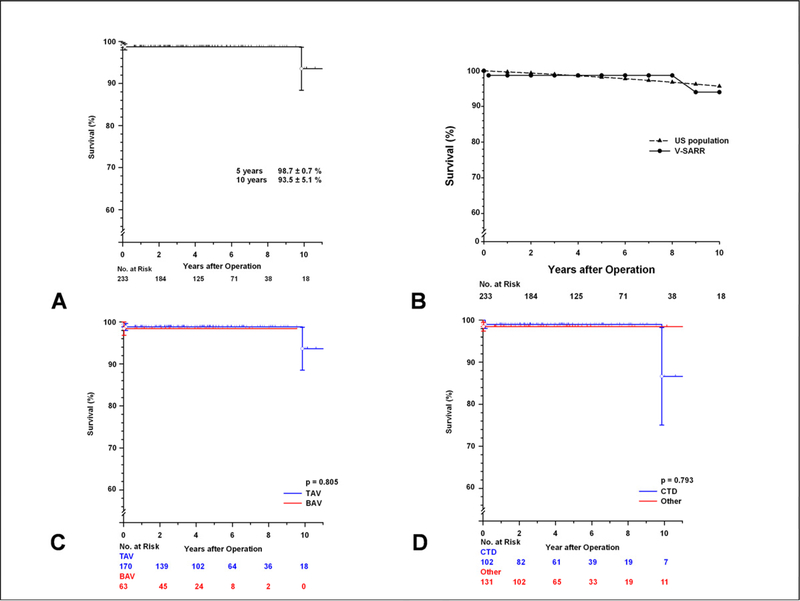
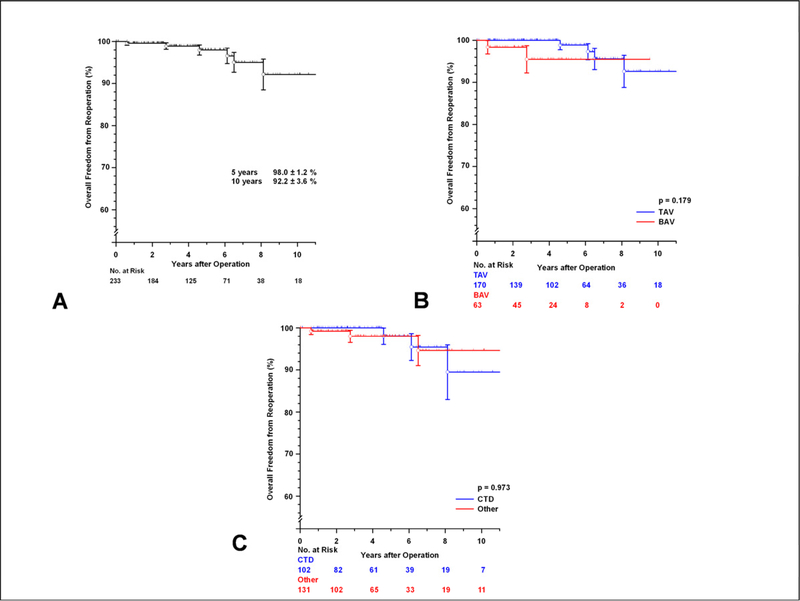
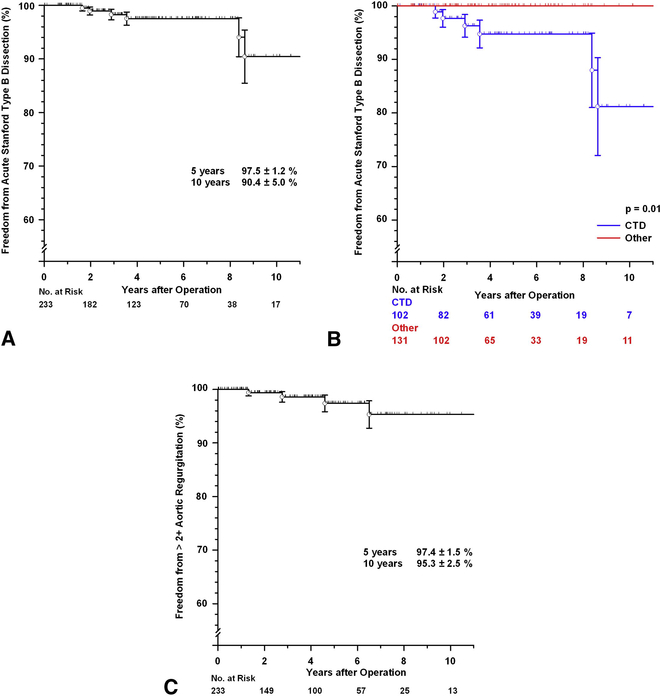
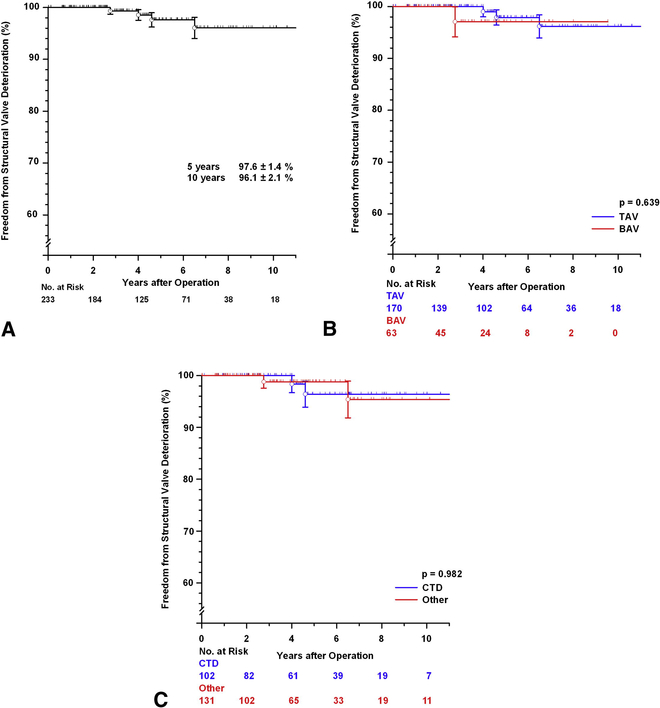
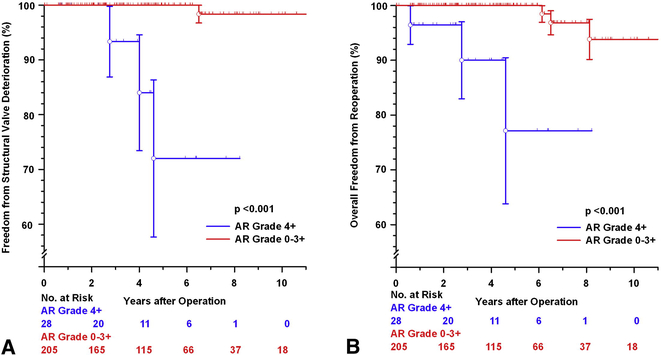
Results: Survival at 5 and 10 years was 98.7% ± 0.7% and 93.5% ± 5.1%, respectively. Freedom from reoperation (all causes) on the aortic root was 92.2% ± 3.6% at 10 years; 3 reoperations were aortic valve replacement owing to structural valve deterioration. Freedom from structural valve deterioration at 10 years was 96.1% ± 2.1%. No significant differences were found in survival (P = .805, P = .793, respectively), reoperation (P = .179, P = .973, respectively), structural valve deterioration (P = .639, P = .982, respectively), or any other functional or clinical endpoints when patients were stratified by valve type (tricuspid aortic valve vs bicuspid aortic valve) or associated connective tissue disorder. At the latest echocardiographic follow-up (95% complete), 202 patients (94.8%) had none or trace aortic regurgitation, 10 (4.7%) mild, 0 had moderate to severe, and 1 (0.5%) had severe aortic regurgitation. Freedom from greater than 2+ aortic regurgitation at 10 years was 95.3% ± 2.5%. Six patients sustained acute type B aortic dissection (freedom at 10 years, 90.4% ± 5.0%).
Conclusions: Tirone David reimplantation valve-sparing aortic root replacement in carefully selected young patients was associated with excellent clinical and echocardiographic outcome in patients with either a tricuspid aortic valve or bicuspid aortic valve. No demonstrable adverse influence was found for Marfan syndrome or connective tissue disorder on durability, clinical outcome, or echocardiographic results.
Copyright © 2013 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Incidence and progression of mild aortic regurgitation after Tirone David reimplantation valve-sparing aortic root replacement.J Thorac Cardiovasc Surg. 2014 Jan;147(1):169-77, 178.e1-178.e3. doi: 10.1016/j.jtcvs.2013.09.009. Epub 2013 Oct 29. J Thorac Cardiovasc Surg. 2014. PMID: 24176278
-
Tirone David valve-sparing aortic root replacement and cusp repair for bicuspid aortic valve disease.J Thorac Cardiovasc Surg. 2013 Mar;145(3 Suppl):S35-40.e1-2. doi: 10.1016/j.jtcvs.2012.11.043. Epub 2012 Dec 20. J Thorac Cardiovasc Surg. 2013. PMID: 23260433
-
David operation: single center 10-year experience.J Cardiovasc Surg (Torino). 2015 Aug;56(4):639-45. Epub 2013 Dec 17. J Cardiovasc Surg (Torino). 2015. PMID: 24343372
-
Valve-sparing aortic root surgery in children and adults with congenital heart disease.J Thorac Cardiovasc Surg. 2021 Sep;162(3):955-962. doi: 10.1016/j.jtcvs.2020.08.116. Epub 2020 Sep 28. J Thorac Cardiovasc Surg. 2021. PMID: 33139062 Review. No abstract available.
-
Current trends in minimally invasive valve-sparing aortic root replacement-Best available evidence.J Card Surg. 2022 Jun;37(6):1684-1690. doi: 10.1111/jocs.16453. Epub 2022 Mar 29. J Card Surg. 2022. PMID: 35348237 Review.
Cited by
-
Toward standardization of valve-sparing root replacement and annuloplasty.Gen Thorac Cardiovasc Surg. 2018 Dec;66(12):685-691. doi: 10.1007/s11748-018-1015-x. Epub 2018 Sep 17. Gen Thorac Cardiovasc Surg. 2018. PMID: 30225772 Review.
-
Early results after aortic annuloplasty with a complete external Dacron band.Gen Thorac Cardiovasc Surg. 2022 Apr;70(4):329-336. doi: 10.1007/s11748-021-01695-1. Epub 2021 Sep 20. Gen Thorac Cardiovasc Surg. 2022. PMID: 34542798 Free PMC article.
-
The Prevalence of Coronary Artery Disease in Bicuspid Aortic Valve Patients: An Overview of the Literature.Aorta (Stamford). 2023 Dec;11(6):191-197. doi: 10.1055/s-0044-1785190. Epub 2024 May 2. Aorta (Stamford). 2023. PMID: 38698623 Free PMC article.
-
Progression of Aortic Regurgitation After Different Repair Techniques for Congenital Aortic Valve Stenosis.Pediatr Cardiol. 2016 Jan;37(1):84-9. doi: 10.1007/s00246-015-1243-0. Epub 2015 Aug 13. Pediatr Cardiol. 2016. PMID: 26266328
-
The Ross procedure and valve-sparing root replacement procedures in the adult patient: do guidelines follow the evidence?Ann Cardiothorac Surg. 2021 Jul;10(4):433-443. doi: 10.21037/acs-2021-rp-24. Ann Cardiothorac Surg. 2021. PMID: 34422555 Free PMC article. Review.
References
-
- Miller DC. Valve-sparing aortic root replacement: current state of the art and where are we headed? Ann Thorac Surg 2007;83:S736–9; - PubMed
-
- Sarsam MA, Yacoub M. Remodeling of the aortic valve anulus. J Thorac Cardiovasc Surg 1993;105:435–8. - PubMed
-
- David TE, Feindel CM. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg 1992;103:617–21; - PubMed
-
- Kallenbach K, Karck M, Pak D, Salcher R, Khaladj N, Leyh R, et al. Decade of aortic valve sparing reimplantation: are we pushing the limits too far? Circulation 2005;112:I253–9. - PubMed
-
- Zehr KJ, Thubrikar MJ, Gong GG, Headrick JR, Robicsek F. Clinical introduction of a novel prosthesis for valve-preserving aortic root reconstruction for annuloaortic ectasia. J Thorac Cardiovasc Surg 2000;120:692–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
