

Does surgery improve outcomes for esophageal squamous cell carcinoma? An analysis using the surveillance epidemiology and end results registry from 1998 to 2008
- PMID: 23084493
- PMCID: PMC3479433
- DOI: 10.1016/j.jamcollsurg.2012.07.006
Does surgery improve outcomes for esophageal squamous cell carcinoma? An analysis using the surveillance epidemiology and end results registry from 1998 to 2008
Abstract
Background: We examined survival associated with locally advanced esophageal squamous cell cancer (SCC) to evaluate if treatment without surgery could be considered adequate.
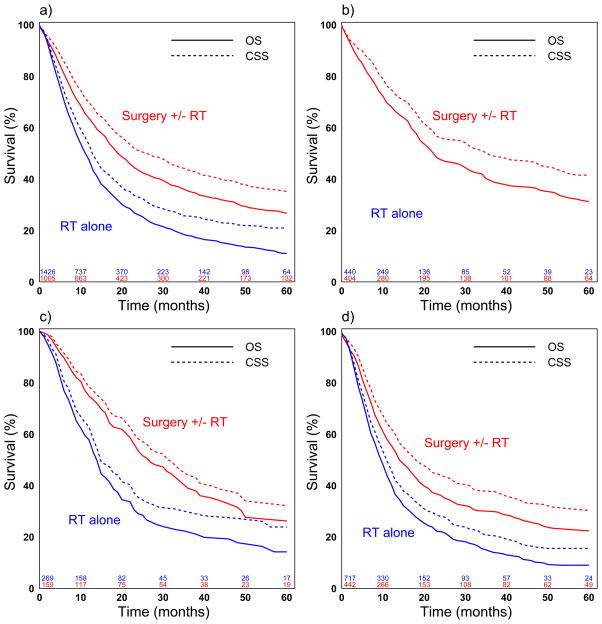
Study design: Patients in the Surveillance, Epidemiology and End Results Registry (SEER) registry with stage II-III SCC of the mid or distal esophagus from 1998-2008 were grouped by treatment with definitive radiation versus esophagectomy with or without radiation. Information on chemotherapy is not recorded in SEER. Tumor stage was defined as first clinical tumor stage in case of neo-adjuvant therapy and pathological report if no neo-adjuvant therapy was performed. Cancer-specific (CSS) and overall survival (OS) were analyzed using the Kaplan-Meier approach and propensity-score adjusted Cox proportional hazard models.
Results: Of the 2,431 patients analyzed, there were 844 stage IIA (34.7%), 428 stage IIB (17.6%), 1,159 stage III (47.7%) patients. Most were treated with definitive radiation (n = 1,426, 58.7%). Of the 1,005 (41.3%) patients who underwent surgery, 369 (36.7%) had preoperative radiation, 160 (15.9%) had postoperative radiation, and 476 (47.4%) had no radiation. Five-year survival was 17.9% for all patients, and 22.1%, 18.5%, and 14.5% for stages IIA, IIB, and stage III, respectively. Compared to treatment that included surgery, definitive radiation alone predicted worse propensity-score adjusted survival for all patients (CSS Hazard Ratio [HR] 1.48, p < 0.001; OS HR 1.46, p < 0.001) and for stage IIA, IIB, and III patients individually (all p values ≤ 0.01). Compared to surgery alone, surgery with radiation predicted improved survival for stage III patients (CSS HR 0.62, p = 0.001, OS HR 0.62, p < 0.001) but not stage IIA or IIB (all p values > 0.18).
Conclusions: Esophagectomy is associated with improved survival for patients with locally advanced SCC and should be considered as an integral component of the treatment algorithm if feasible.
Copyright © 2012 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2008. National Cancer Institute; Bethesda, MD: http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER web site, 2011.
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349(23):2241–52. - PubMed
-
- Pennathur A, Luketich JD. Resection for esophageal cancer: strategies for optimal management. Ann Thorac Surg. 2008;85(2):S751–6. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29. - PubMed
-
- Dubecz A, Gall I, Solymosi N, et al. Temporal trends in long-term survival and cure rates in esophageal cancer: a SEER database analysis. J Thorac Oncol. 2012;7(2):443–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
