

Association of circulating fibroblast growth factor-23 with renal phosphate excretion among hemodialysis patients with residual renal function
- PMID: 23085728
- PMCID: PMC3531650
- DOI: 10.2215/CJN.00230112
Association of circulating fibroblast growth factor-23 with renal phosphate excretion among hemodialysis patients with residual renal function
Abstract
Background and objectives: High serum levels of fibroblast growth factor-23 (FGF-23) are associated with mortality in patients with ESRD, but whether it still acts as a phosphaturic factor is unknown. This study aimed to explore the role of circulating FGF-23 on urinary phosphate excretion and phosphate balance in maintenance hemodialysis (MHD) patients with residual renal function (RRF).
Design, setting, participants, & measurements: There were 134 MHD patients enrolled in this cross-sectional study from June to July 2010. Demographics, laboratory data, and excretion capacity of phosphate were recorded. Multivariable linear regression was used to analyze the relationship of serum phosphate and the tubular reabsorption rate of phosphate with other factors.
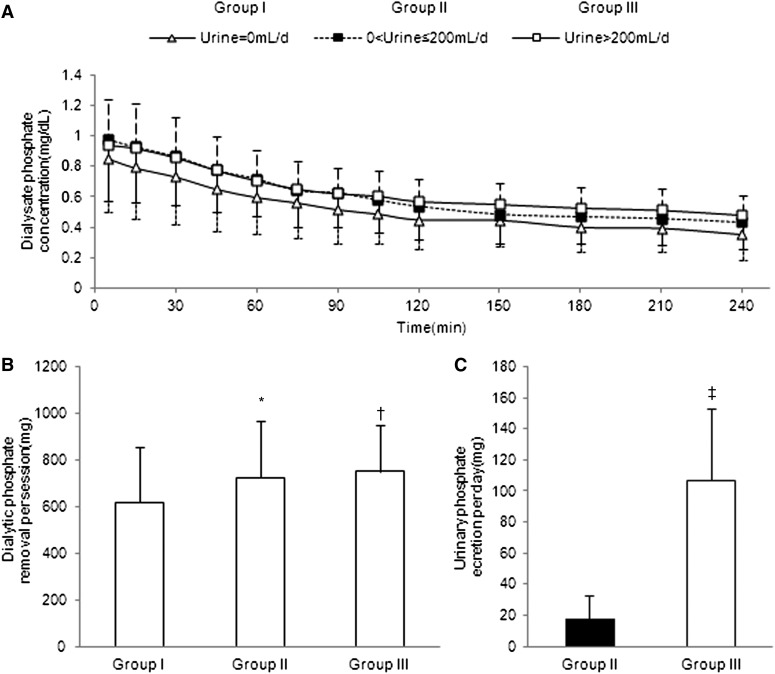
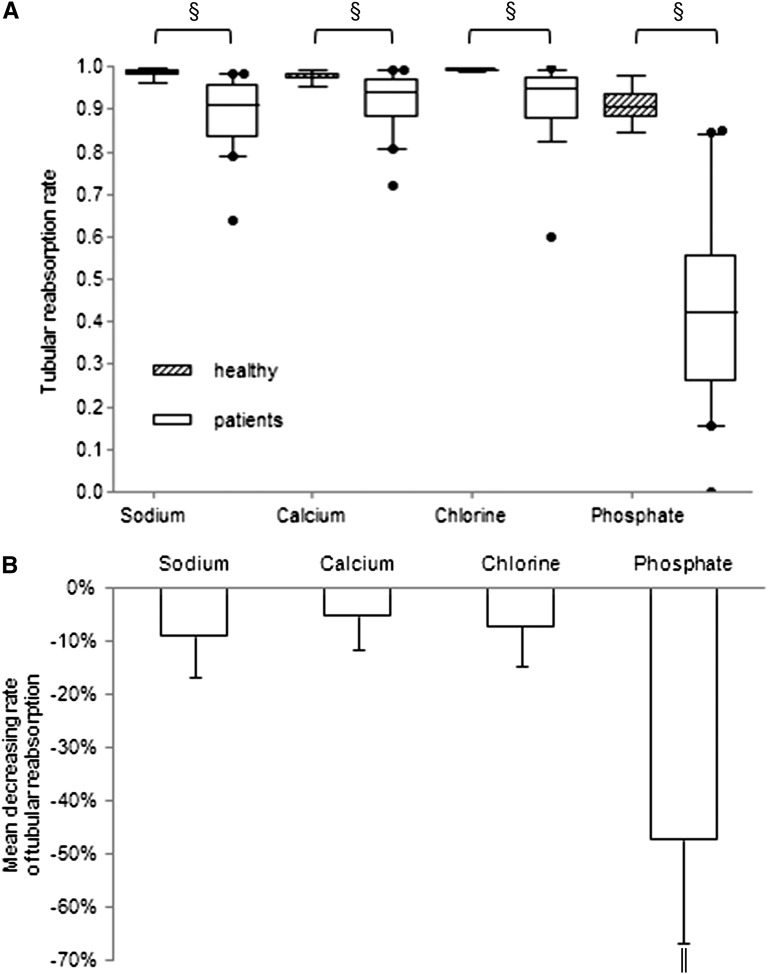
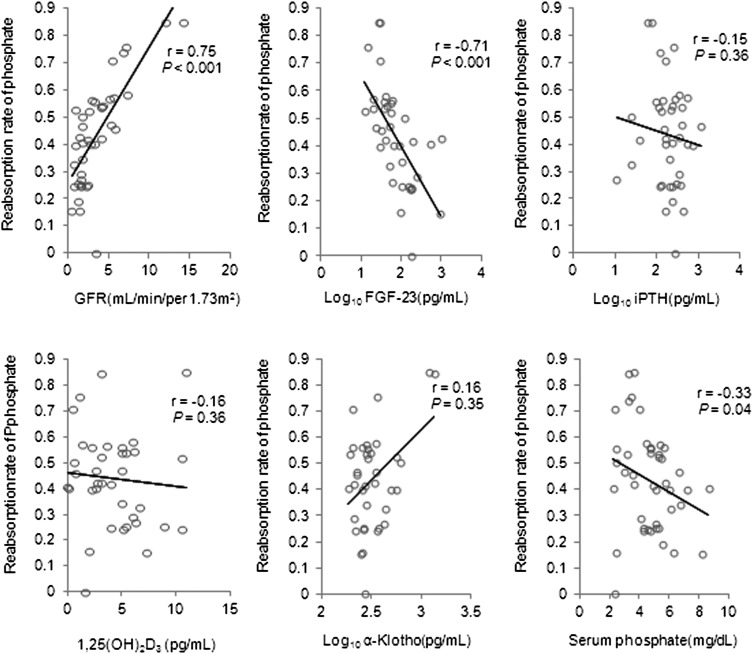
Results: The median age of the patients was 61.0 years and 47.8% were male. Thirty percent of the patients had high urinary output (>200 ml/d) accompanied by lower serum levels of phosphate, calcium, intact parathyroid hormone, and FGF-23 compared with those with low urine output (≤200 ml/d). The independent predictors of serum phosphate were normalized protein nitrogen appearance, intact parathyroid hormone, and FGF-23 in the low urine output group and female sex and GFR in the high urine output group. The tubular reabsorption rate of phosphate decreased to 50% of the normal level in patients with RRF. Elevated circulating FGF-23 was significantly associated with lower tubular phosphate reabsorption after adjusting for GFR.
Conclusions: RRF is associated with significant capacity to excrete phosphate in MHD patients and high levels of serum FGF-23 may promote phosphate excretion by remnant nephrons.
Figures
Similar articles
-
Fibroblast growth factor 23, but not parathyroid hormone, is associated with urinary phosphate regulation in patients on peritoneal dialysis.Ther Apher Dial. 2015 Feb;19(1):73-80. doi: 10.1111/1744-9987.12221. Epub 2014 Sep 4. Ther Apher Dial. 2015. PMID: 25195562
-
Phosphate handling by end-stage kidneys and benefits of residual renal function on phosphate removal in patients on haemodialysis.Nephrology (Carlton). 2013 Apr;18(4):285-91. doi: 10.1111/nep.12039. Nephrology (Carlton). 2013. PMID: 23432763
-
Lower serum fibroblast growth factor-23 levels may suggest malnutrition in maintenance haemodialysis patients.Nephrology (Carlton). 2014 Sep;19(9):568-73. doi: 10.1111/nep.12290. Nephrology (Carlton). 2014. PMID: 24947687
-
Clinical relevance of FGF-23 in chronic kidney disease.Kidney Int Suppl. 2009 Dec;(114):S34-42. doi: 10.1038/ki.2009.405. Kidney Int Suppl. 2009. PMID: 19946326 Review.
-
Regulatory mechanisms of circulating fibroblast growth factor 23 in parathyroid diseases.Ther Apher Dial. 2007 Oct;11 Suppl 1:S32-7. doi: 10.1111/j.1744-9987.2007.00519.x. Ther Apher Dial. 2007. PMID: 17976083 Review.
Cited by
-
Relationship between Residual Urine Output and Type of Dialysis with FGF23 Levels.J Clin Med. 2022 Dec 28;12(1):222. doi: 10.3390/jcm12010222. J Clin Med. 2022. PMID: 36615023 Free PMC article.
-
Significance of residual renal function for phosphate control in chronic hemodialysis patients.Kidney Res Clin Pract. 2014 Mar;33(1):58-64. doi: 10.1016/j.krcp.2014.01.001. Epub 2014 Mar 12. Kidney Res Clin Pract. 2014. PMID: 26885471 Free PMC article.
-
Twice-weekly and incremental hemodialysis treatment for initiation of kidney replacement therapy.Am J Kidney Dis. 2014 Aug;64(2):181-6. doi: 10.1053/j.ajkd.2014.04.019. Epub 2014 May 17. Am J Kidney Dis. 2014. PMID: 24840669 Free PMC article. Review.
-
Infrequent dialysis: a new paradigm for hemodialysis initiation.Semin Dial. 2013 Nov-Dec;26(6):720-7. doi: 10.1111/sdi.12133. Epub 2013 Sep 9. Semin Dial. 2013. PMID: 24016197 Free PMC article. Review.
-
Health care providers' support of patients' autonomy, phosphate medication adherence, race and gender in end stage renal disease.J Behav Med. 2016 Dec;39(6):1104-1114. doi: 10.1007/s10865-016-9745-7. Epub 2016 May 11. J Behav Med. 2016. PMID: 27167227 Free PMC article.
References
-
- Tentori F: Mineral and bone disorder and outcomes in hemodialysis patients: Results from the DOPPS. Semin Dial 23: 10–14, 2010 - PubMed
-
- Wang AY, Woo J, Sea MM, Law MC, Lui SF, Li PK: Hyperphosphatemia in Chinese peritoneal dialysis patients with and without residual kidney function: What are the implications? Am J Kidney Dis 43: 712–720, 2004 - PubMed
-
- Penne EL, van der Weerd NC, Grooteman MP, Mazairac AH, van den Dorpel MA, Nubé MJ, Bots ML, Lévesque R, ter Wee PM, Blankestijn PJ, CONTRAST investigators : Role of residual renal function in phosphate control and anemia management in chronic hemodialysis patients. Clin J Am Soc Nephrol 6: 281–289, 2011 - PMC - PubMed
-
- Murer H, Hernando N, Forster I, Biber J: Proximal tubular phosphate reabsorption: Molecular mechanisms. Physiol Rev 80: 1373–1409, 2000 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
