

Adaptive dosing approaches to the individualization of 13-cis-retinoic acid (isotretinoin) treatment for children with high-risk neuroblastoma
- PMID: 23087409
- PMCID: PMC3548903
- DOI: 10.1158/1078-0432.CCR-12-2225
Adaptive dosing approaches to the individualization of 13-cis-retinoic acid (isotretinoin) treatment for children with high-risk neuroblastoma
Abstract
Purpose: To investigate the feasibility of adaptive dosing and the impact of pharmacogenetic variation on 13-cis-retinoic acid (13-cisRA) disposition in high-risk patients with neuroblastoma.
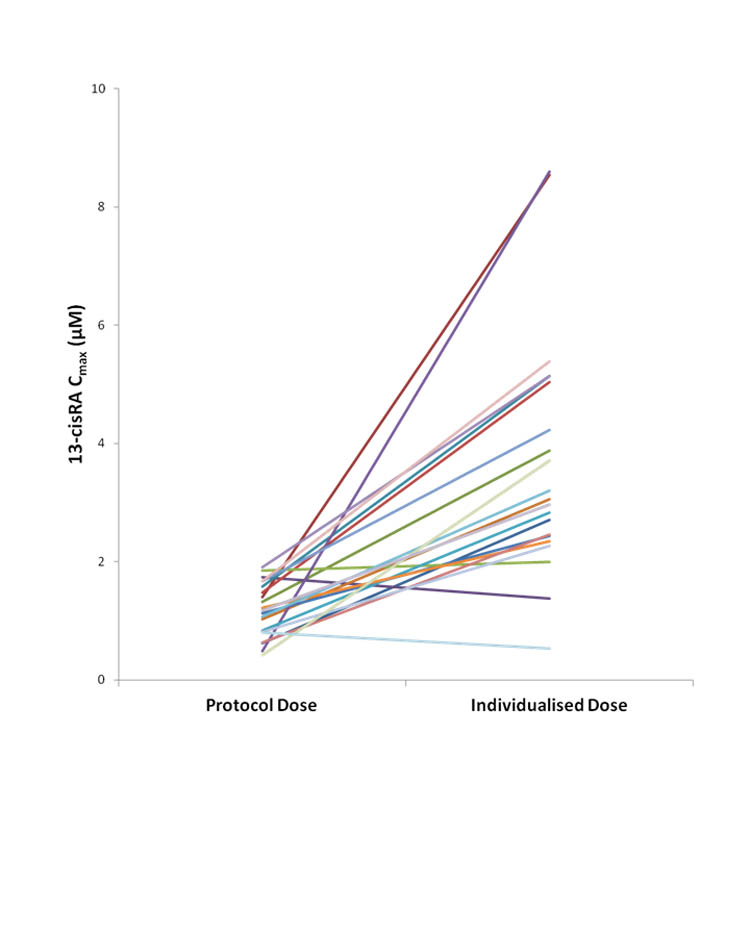
Experimental design: 13-cisRA (160 mg/m(2) or 5.33 mg/kg/d) was administered to 103 patients ages 21 years or less and plasma concentrations of 13-cisRA and 4-oxo-13-cisRA quantitated on day 14 of treatment. Seventy-one patients were recruited to a dose adjustment group, targeting a 13-cisRA C(max) of 2 μmol/L, with dose increases of 25% to 50% implemented for patients with C(max) values less than 2 μmol/L. A population pharmacokinetic model was applied and polymorphisms in relevant cytochrome P450 genes analyzed.
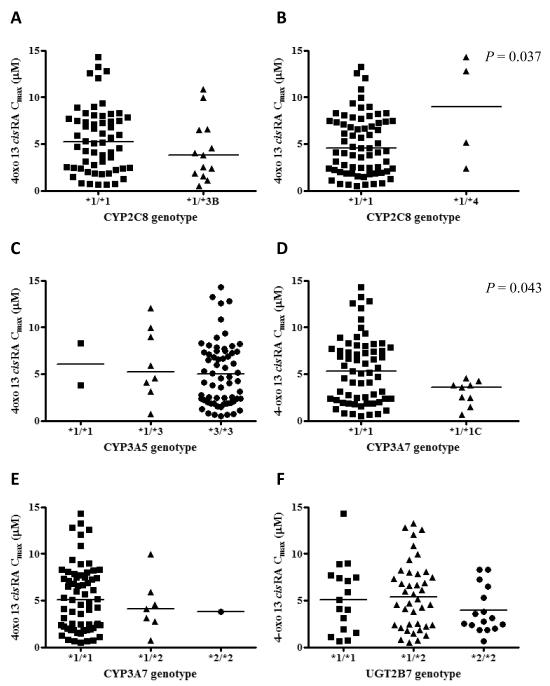
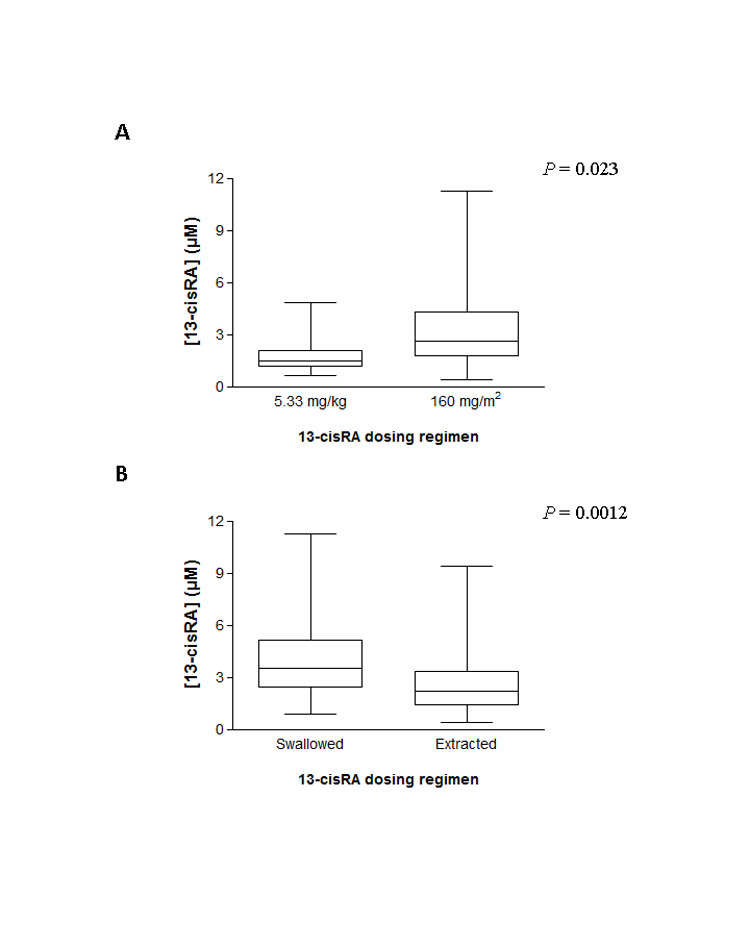
Results: 13-cisRA C(max) values ranged from 0.42 to 11.2 μmol/L, with 34 of 103 (33%) patients failing to achieve a C(max) more than 2 μmol/L. Dose increases carried out in 20 patients in the dose adjustment study group led to concentrations more than 2 μmol/L in 18 patients (90%). Eight of 11 (73%) patients less than 12 kg, receiving a dose of 5.33 mg/kg, failed to achieve a C(max) of 2 μmol/L or more. Significantly, lower C(max) values were observed for patients treated with 5.33 mg/kg versus 160 mg/m(2) (1.9 ± 1.2 vs. 3.1 ± 2.0 μmol/L; mean ± SD; P = 0.023). C(max) was higher in patients who swallowed 13-cisRA capsules as compared with receiving the drug extracted from capsules (4.0 ± 2.2 vs. 2.6 ± 1.8 μmol/L; P = 0.0012). The target C(max) was achieved by 93% (25/27) versus 55% (42/76) of patients in these 2 groups, respectively. No clear relationships were found between genetic variants and 13-cisRA pharmacokinetic parameters.
Conclusions: Dosing regimen and method of administration have a marked influence on 13-cisRA plasma concentrations. Body weight-based dosing should not be implemented for children less than 12 kg and pharmacologic data support higher doses for children unable to swallow 13-cisRA capsules.
©2012 AACR.
Figures
Comment in
-
Targeted isotretinoin in neuroblastoma: kinetics, genetics, or absorption.Clin Cancer Res. 2013 Jan 15;19(2):311-3. doi: 10.1158/1078-0432.CCR-12-3313. Epub 2012 Dec 3. Clin Cancer Res. 2013. PMID: 23209029 Free PMC article.
References
-
- Matthay KK, Villablanca JG, Seeger RC, Stram DO, Harris RE, Ramsay NK, et al. Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation, and 13-cis-retinoic acid. Children’s Cancer Group. N Engl J Med. 1999;341:1165–73. - PubMed
-
- Matthay KK, Reynolds CP, Seeger RC, Shimada H, Adkins ES, Haas-Kogan D, et al. Long-term results for children with high-risk neuroblastoma treated on a randomized trial of myeloablative therapy followed by 13-cis-retinoic acid: a Children’s Oncology Group study. J Clin Oncol. 2009;27:1007–13. - PMC - PubMed
-
- van der Leede BM, van den Brink CE, Pijnappel WWM, Sonneveld E, van der Saag PT, van der Berg B. Autoinduction of retinoic acid metabolism to polar derivatives with decreased biological activity in retinoic acid-sensitive, but not in retinoic acid resistant human breast cancer cells. J Biol Chem. 1997;272:17921–8. - PubMed
-
- Kim SY, Yoo SJ, Kwon HJ, Kim SH, Byun Y, Lee K-S. Retinoic acid 4-hydroxylase-mediated catabolism of all-trans retinoic acid and the cell proliferation in head and neck squamous cell carcinoma. Metabolism. 2002;51:477–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
