Spontaneous reduction of prolactinoma post cabergoline withdrawal
- PMID: 23087877
- PMCID: PMC3475917
- DOI: 10.4103/2230-8210.100656
Spontaneous reduction of prolactinoma post cabergoline withdrawal
Abstract
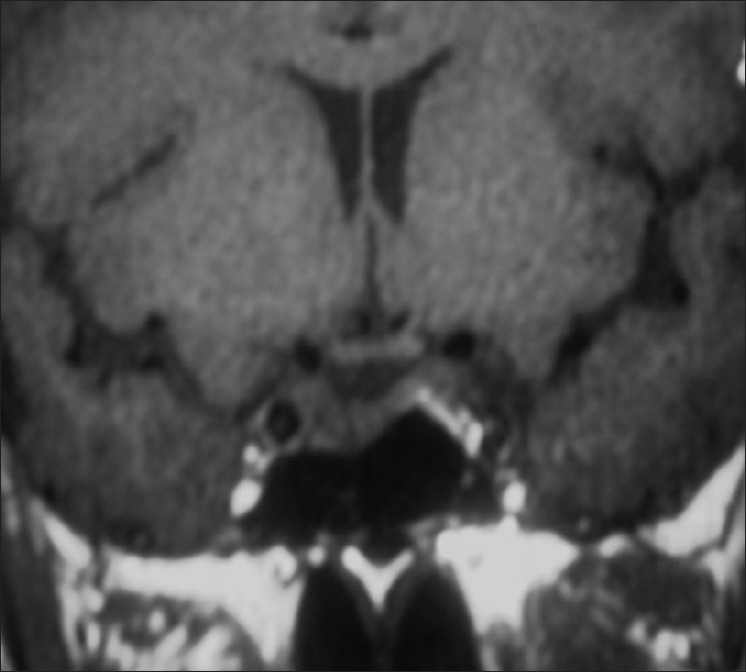
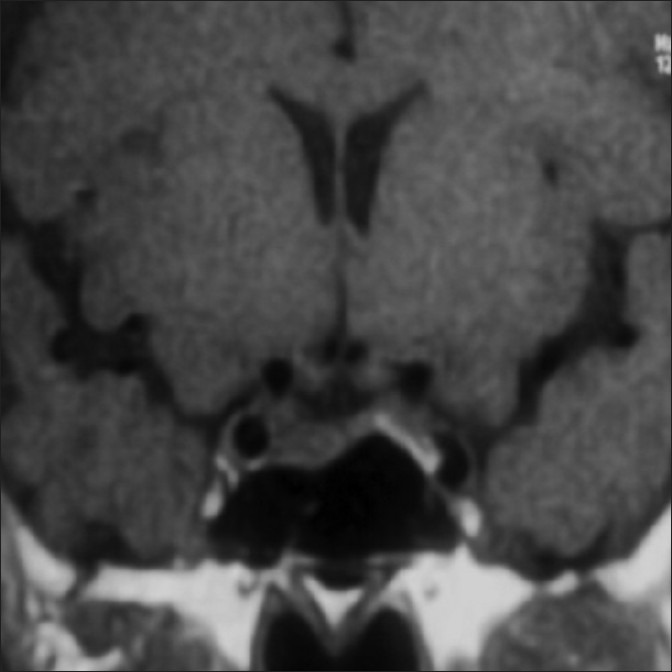
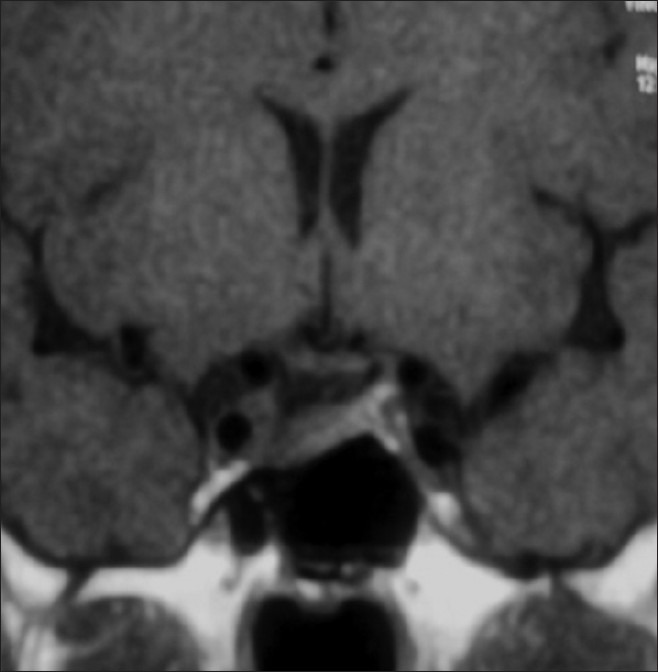
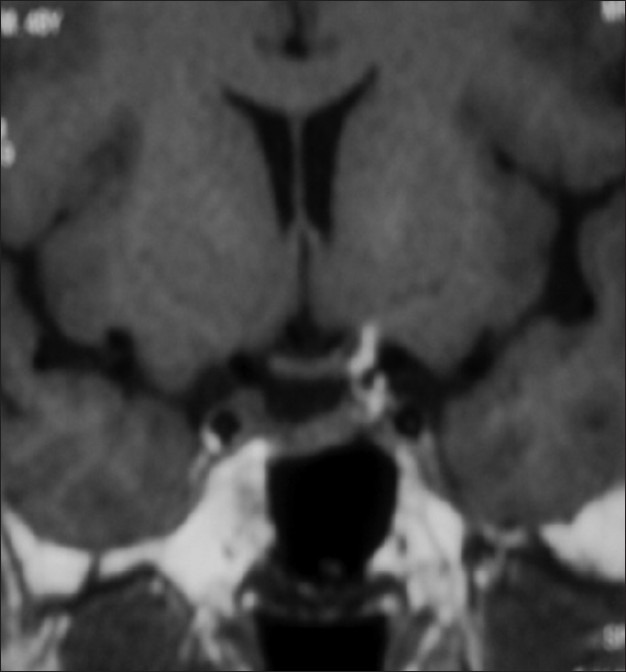
Prolactinomas are common pituitary tumors usually highly responsive to dopamine agonists. Around 70-90% of the prolactinomas exhibit decrease in tumor size, though variably with these agents. Uncommonly, there may be little or no shrinkage in pituitary tumor. In the absence of medical therapy, pituitary apoplexy may also result in tumor shrinkage, albeit rarely. We report here a case showing only modest reduction in prolactinoma with cabergoline given for a period of one and a half years. Surprisingly, this tumor showed a 40% reduction in the tumor size 3 months after cabergoline withdrawal in the absence of clinical or radiological evidence of apoplexy.
Keywords: Cabergoline withdrawal; prolactinoma; spontaneous involution.
Conflict of interest statement
Figures
Similar articles
-
Hormone levels and tumour size response to quinagolide and cabergoline in patients with prolactin-secreting and clinically non-functioning pituitary adenomas: predictive value of pituitary scintigraphy with 123I-methoxybenzamide.Clin Endocrinol (Oxf). 2000 Apr;52(4):437-45. doi: 10.1046/j.1365-2265.2000.00951.x. Clin Endocrinol (Oxf). 2000. PMID: 10762286 Clinical Trial.
-
Pituitary Apoplexy during Treatment of Prolactinoma with Cabergoline.Asian J Neurosurg. 2018 Jan-Mar;13(1):93-95. doi: 10.4103/1793-5482.181130. Asian J Neurosurg. 2018. PMID: 29492132 Free PMC article.
-
The effect of quinagolide and cabergoline, two selective dopamine receptor type 2 agonists, in the treatment of prolactinomas.Clin Endocrinol (Oxf). 2000 Jul;53(1):53-60. doi: 10.1046/j.1365-2265.2000.01016.x. Clin Endocrinol (Oxf). 2000. PMID: 10931080 Clinical Trial.
-
Dopamine agonists in prolactinomas: when to withdraw?Pituitary. 2020 Feb;23(1):38-44. doi: 10.1007/s11102-019-00989-1. Pituitary. 2020. PMID: 31556013 Review.
-
Hyperprolactinemia/Prolactinomas in the Postmenopausal Period: Challenges in Diagnosis and Management.Neuroendocrinology. 2019;109(1):28-33. doi: 10.1159/000494725. Epub 2018 Oct 22. Neuroendocrinology. 2019. PMID: 30347396 Review.
References
-
- Molitch ME, Elton RL, Blackwell RE, Caldwell B, Chang RJ, Jaffe R, et al. Bromocriptine as primary therapy for prolactin-secreting macroadenomas: Results of a prospective multicenter study. J Clin Endocrinol Metab. 1985;60:698–705. - PubMed
-
- Webster J, Piscitelli G, Polli A, Ferrari CI, Ismail I, Scanlon MF. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea.Cabergoline Comparative Study Group. N Engl J Med. 1994;331:904–9. - PubMed
-
- Olafsdottir A, Schlechte J. Management of resistant prolactinomas. Nat Clin Pract Endocrinol Metab. 2006;2:552–61. - PubMed
-
- Molich ME. Pharmacological resistance in prolactinoma patients. Pituitary. 2005;8:43–52. - PubMed
-
- Iván G, Szigeti-Csúcs N, Oláh M, Nagy GM, Góth MI. Treatment of pituitary tumors: Dopamine agonists. Endocrine. 2005;28:101–10. - PubMed