

Individual and institutional determinants of caesarean section in referral hospitals in Senegal and Mali: a cross-sectional epidemiological survey
- PMID: 23088501
- PMCID: PMC3534628
- DOI: 10.1186/1471-2393-12-114
Individual and institutional determinants of caesarean section in referral hospitals in Senegal and Mali: a cross-sectional epidemiological survey
Abstract
Background: Two years after implementing the free-CS policy, we assessed the non-financial factors associated with caesarean section (CS) in women managed by referral hospitals in Senegal and Mali.
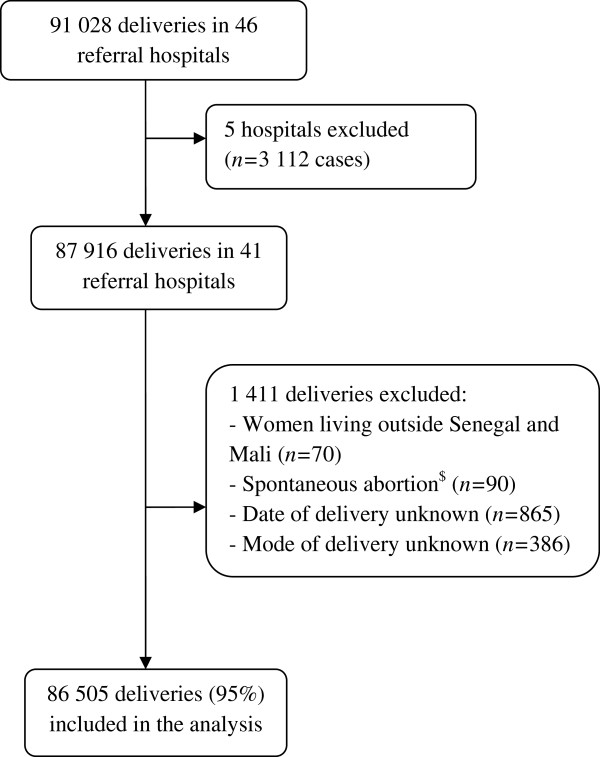
Methods: We conducted a cross-sectional survey nested in a cluster trial (QUARITE trial) in 41 referral hospitals in Senegal and Mali (10/01/2007-10/01/2008). Data were collected regarding women's characteristics and on available institutional resources. Individual and institutional factors independently associated with emergency (before labour), intrapartum and elective CS were determined using a hierarchical logistic mixed model.
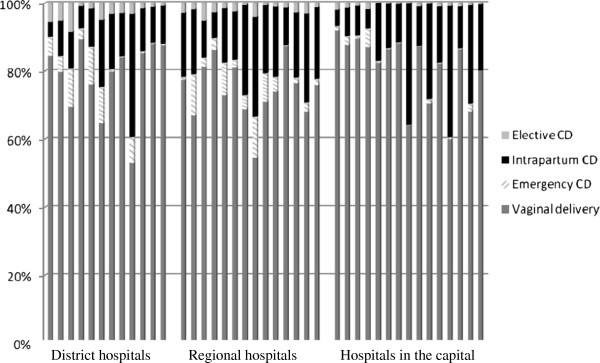
Results: Among 86 505 women, 14% delivered by intrapartum CS, 3% by emergency CS and 2% by elective CS. For intrapartum, emergency and elective CS, the main maternal risk factors were, respectively: previous CS, referral from another facility and suspected cephalopelvic-disproportion (adjusted Odds Ratios from 2.8 to 8.9); vaginal bleeding near full term, hypertensive disorders, previous CS and premature rupture of membranes (adjusted ORs from 3.9 to 10.2); previous CS (adjusted OR=19.2 [17.2-21.6]). Access to adult and neonatal intensive care, a 24-h/day anaesthetist and number of annual deliveries per hospital were independent factors that affected CS rates according to degree of urgency. The presence of obstetricians and/or medical-anaesthetists was associated with an increased risk of elective CS (adjusted ORs [95%CI] = 4.8 [2.6-8.8] to 9.4 [5.1-17.1]).
Conclusions: We confirm the significant effect of well-known maternal risk factors affecting the mode of delivery. Available resources at the institutional level and the degree of urgency of CS should be taken into account in analysing CS rates in this context.
Figures
Similar articles
-
Maternal and perinatal outcomes by mode of delivery in senegal and mali: a cross-sectional epidemiological survey.PLoS One. 2012;7(10):e47352. doi: 10.1371/journal.pone.0047352. Epub 2012 Oct 8. PLoS One. 2012. PMID: 23056633 Free PMC article.
-
Factors associated with postpartum hemorrhage maternal death in referral hospitals in Senegal and Mali: a cross-sectional epidemiological survey.BMC Pregnancy Childbirth. 2015 Sep 30;15:235. doi: 10.1186/s12884-015-0669-y. BMC Pregnancy Childbirth. 2015. PMID: 26423997 Free PMC article.
-
Predicting in-hospital maternal mortality in Senegal and Mali.PLoS One. 2013 May 30;8(5):e64157. doi: 10.1371/journal.pone.0064157. Print 2013. PLoS One. 2013. PMID: 23737972 Free PMC article.
-
Quality of care, risk management, and technology in obstetrics to reduce hospital-based maternal mortality in Senegal and Mali (QUARITE): a cluster-randomised trial.Lancet. 2013 Jul 13;382(9887):146-57. doi: 10.1016/S0140-6736(13)60593-0. Epub 2013 May 28. Lancet. 2013. PMID: 23721752 Clinical Trial.
-
Maternal and perinatal outcomes associated with a trial of labour after previous caesarean section in sub-Saharan countries.BJOG. 2016 Dec;123(13):2147-2155. doi: 10.1111/1471-0528.13615. Epub 2015 Sep 16. BJOG. 2016. PMID: 26374554
Cited by
-
DECIDE: a cluster randomized controlled trial to reduce non-medically indicated caesareans in Burkina Faso.BMC Pregnancy Childbirth. 2016 Oct 21;16(1):322. doi: 10.1186/s12884-016-1112-8. BMC Pregnancy Childbirth. 2016. PMID: 27769190 Free PMC article. Clinical Trial.
-
Cesarean section in sub-Saharan Africa.Matern Health Neonatol Perinatol. 2016 Jul 8;2:6. doi: 10.1186/s40748-016-0033-x. eCollection 2016. Matern Health Neonatol Perinatol. 2016. PMID: 27398224 Free PMC article. Review.
-
How does hospital organisation influence the use of caesarean sections in low- and middle-income countries? A cross-sectional survey in Argentina, Burkina Faso, Thailand and Vietnam for the QUALI-DEC project.BMC Pregnancy Childbirth. 2024 Jan 17;24(1):67. doi: 10.1186/s12884-024-06257-w. BMC Pregnancy Childbirth. 2024. PMID: 38233792 Free PMC article.
-
Disparities in caesarean section prevalence and determinants across sub-Saharan Africa countries.Glob Health Res Policy. 2018 Jul 2;3:19. doi: 10.1186/s41256-018-0074-y. eCollection 2018. Glob Health Res Policy. 2018. PMID: 29988650 Free PMC article.
-
Prevalence and determinants of caesarean section deliveries in the Kintampo Districts of Ghana.BMC Pregnancy Childbirth. 2023 Apr 25;23(1):286. doi: 10.1186/s12884-023-05622-5. BMC Pregnancy Childbirth. 2023. PMID: 37098478 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
