

Hematopoietic cell transplantation with cord blood for cure of HIV infections
- PMID: 23089564
- PMCID: PMC4651173
- DOI: 10.1016/j.bbmt.2012.10.017
Hematopoietic cell transplantation with cord blood for cure of HIV infections
Abstract
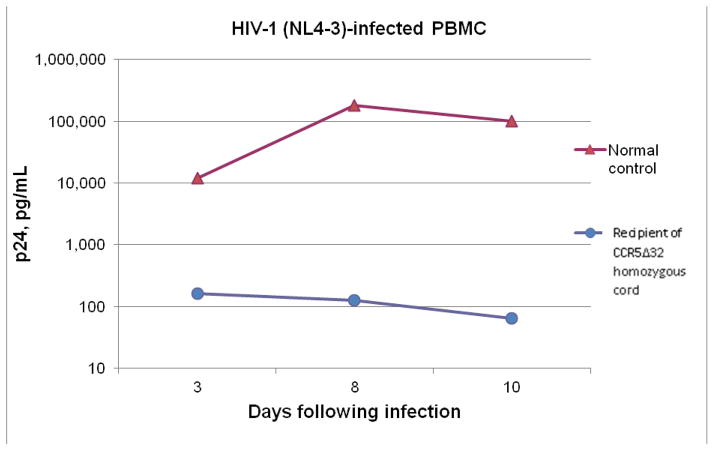
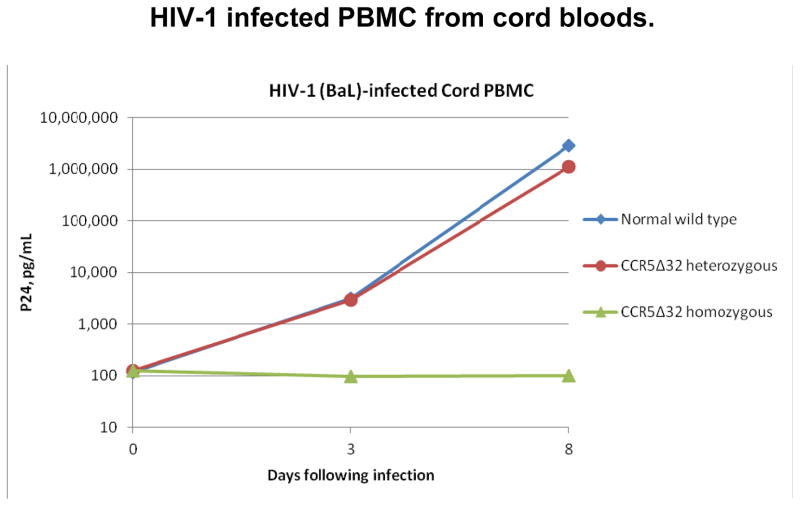
Hematopoietic cell transplantation (HCT) using CCR5-Δ32/Δ32 stem cells from an adult donor has resulted in the only known cure of human immunodeficiency virus (HIV) infection. However, it is not feasible to repeat this procedure except rarely because of the low incidence of the CCR5-Δ32 allele, the availability of only a small number of potential donors for most patients, and the need for a very close human leukocyte antigen (HLA) match between adult donors and recipients. In contrast, cord blood (CB) transplantations require significantly less stringent HLA matching. Therefore, our hypothesis is that cure of HIV infections by HCT can be accomplished much more readily using umbilical CB stem cells obtained from a modestly sized inventory of cryopreserved CCR5-Δ32/Δ32 CB units. To test this hypothesis, we developed a screening program for CB units and are developing an inventory of CCR5-Δ32/Δ32 cryopreserved units available for HCT. Three hundred such units are projected to provide for white pediatric patients a 73.6% probability of finding an adequately HLA matched unit with a cell dose of ≥2.5 × 10(7) total nucleated cells (TNCs)/kg and a 27.9% probability for white adults. With a cell dose of ≥1 × 10(7) TNCs/kg, the corresponding projected probabilities are 85.6% and 82.1%. The projected probabilities are lower for ethnic minorities. Impetus for using CB HCT was provided by a transplantation of an adult with acute myelogenous leukemia who was not HIV infected. The HCT was performed with a CCR5-Δ32/Δ32 CB unit, and posttransplantation in vitro studies indicated that the patient's peripheral blood mononuclear cells were resistant to HIV infection.
Copyright © 2013 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures:
L.P., D.S., R.T., S,S., A.B., and R.C. were employees of StemCyte International Cord Blood Center (“StemCyte”) while this work was being done. L.P., R.T. and S.S are still employed by StemCyte. L.P. and R.C. have stock options in StemCyte. J.K. is a consultant to StemCyte. The following authors have no conflicts of interest to report: I.R., Y.B., D.R., E.S., J.G., S.Q., P.C., S.S., M.B., L.G., J.R., S.L., H.L., J.R., J.Z. and S.F.
Figures

References
-
- Berger EA, Doms RW, Fenyo EM, et al. A new classification for HIV-1. Nature. 1998;391:240. - PubMed
-
- Samson M, Libert F, Doranz BJ, et al. Resistance to HIV-1 infection in caucasian individuals bearing mutant alleles of the CCR-5 chemokine receptor gene. Nature. 1996;382:722–725. - PubMed
-
- Liu R, Paxton WA, Choe S, et al. Homozygous defect in HIV-1 coreceptor accounts for resistance of some multiply-exposed individuals to HIV-1 infection. Cell. 1996;86:367–377. - PubMed
-
- Hutter G, Nowak E, Mossner M. Long-term control of HIV by CCR5 Delta32/Delta32 stem cell transplantation. New Eng J Med. 2009;360:692–698. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
