

Pelvic fixation for adult scoliosis
- PMID: 23090091
- PMCID: PMC3616465
- DOI: 10.1007/s00586-012-2525-3
Pelvic fixation for adult scoliosis
Abstract
Introduction: Obtaining a fusion, especially to the sacrum for adult deformity correction remains a challenge. Prior to modern fixation techniques, the reported fusion rates for adult scoliotic deformities were low. However sacropelvic fixation techniques for adult deformity continue to evolve. As a result, modern day pelvic fixation techniques have improved fusion rates at the base of long constructs. The purpose of this article is to discuss the history, indications, and modern fixation techniques for pelvic fixation in the surgical management of adult scoliosis patients.
Methods: We searched PUBMED using the search terms pelvic fixation, deformity, lumbopelvic, sacropelvic, and iliac fixation. Linkage or association studies published in English and available full-text were analyzed specifically regarding techniques and innovations in pelvic fixation.
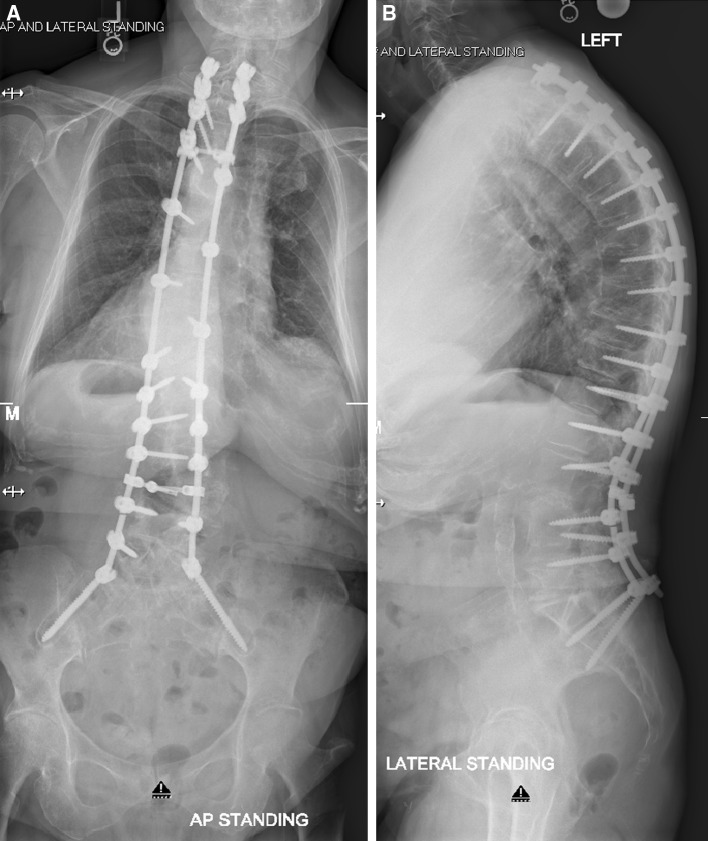
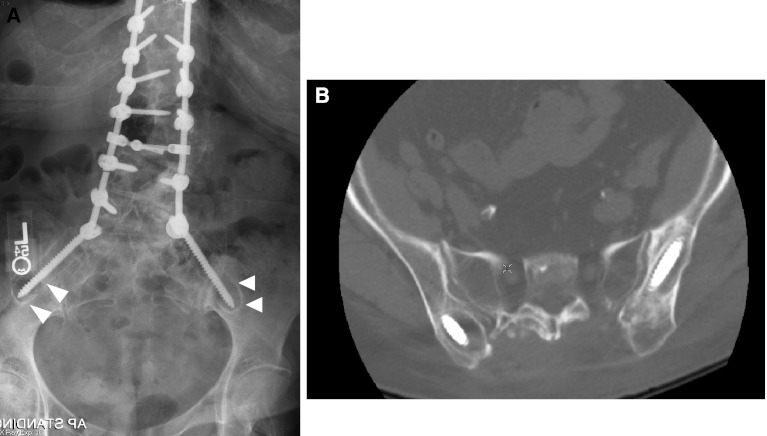
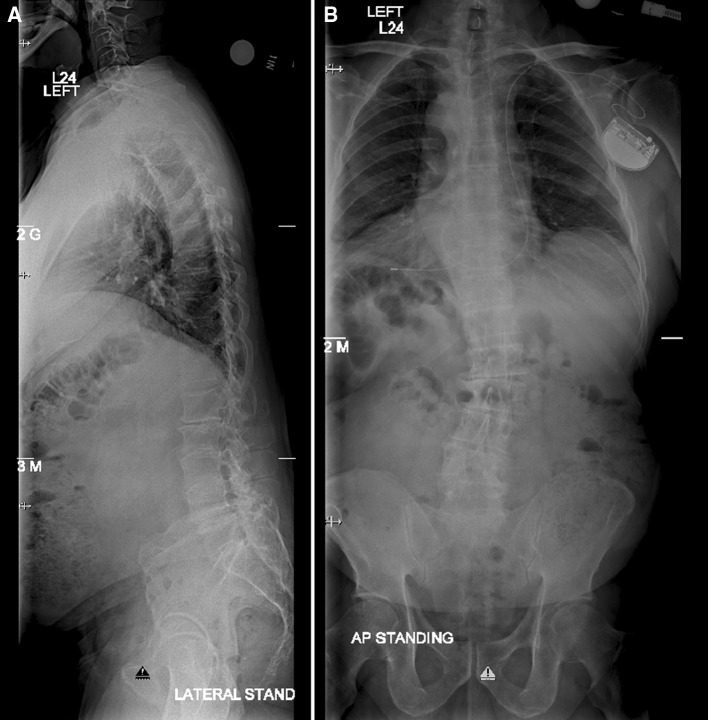
Results: Sacropelvic fixation should be considered in any patient with a long construct ending in the sacrum, those patients with associated risk factors for loss of distal fixation or high risk for pseudarthrosis at L5-S1, and those undergoing three column osteotomies or vertebral body resections in the low lumbar spine. Current pelvic fixation techniques with iliac screws, multiple screw/rod constructs, and S2-alar-iliac screws are all viable techniques for achieving pelvic fixation.
Conclusions: There is growing evidence that pelvic fixation may become the standard for obtaining long fusions in adult scoliosis. Although technically challenging, in selected cases the use of four pelvic screws and/or four rods across the lumbosacral pelvis can help address pseudarthroses, implant breakage, and screw pullout secondary to osteoporosis. Ultimately, indications and techniques should be individualized to the patient and based on surgeon preference and experience.
Figures



References
-
- Bridwell KH, Kuklo T, Edwards CC, II, et al. Sacropelvic Fixation. Memphis: Medtronic Sofamor Danek; 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
