

Volumetric contrast-enhanced ultrasound imaging to assess early response to apoptosis-inducing anti-death receptor 5 antibody therapy in a breast cancer animal model
- PMID: 23091246
- PMCID: PMC3560397
- DOI: 10.7863/jum.2012.31.11.1759
Volumetric contrast-enhanced ultrasound imaging to assess early response to apoptosis-inducing anti-death receptor 5 antibody therapy in a breast cancer animal model
Abstract
Objectives: The objective of this study was to determine whether volumetric contrast-enhanced ultrasound (US) imaging could detect early tumor response to anti-death receptor 5 antibody (TRA-8) therapy alone or in combination with chemotherapy in a preclinical triple-negative breast cancer animal model.
Methods: Animal experiments had Institutional Animal Care and Use Committee approval. Thirty breast tumor-bearing mice were administered Abraxane (paclitaxel; Celgene Corporation, Summit, NJ), TRA-8, TRA-8 + Abraxane, or saline as a controlon days 0, 3, 7, 10, 14, and 17. Volumetric contrast-enhanced US imaging was performedon days 0, 1, 3, and 7 before dosing. Changes in parametric maps of tumor perfusion were compared with the tumor volume and immunohistologic findings.
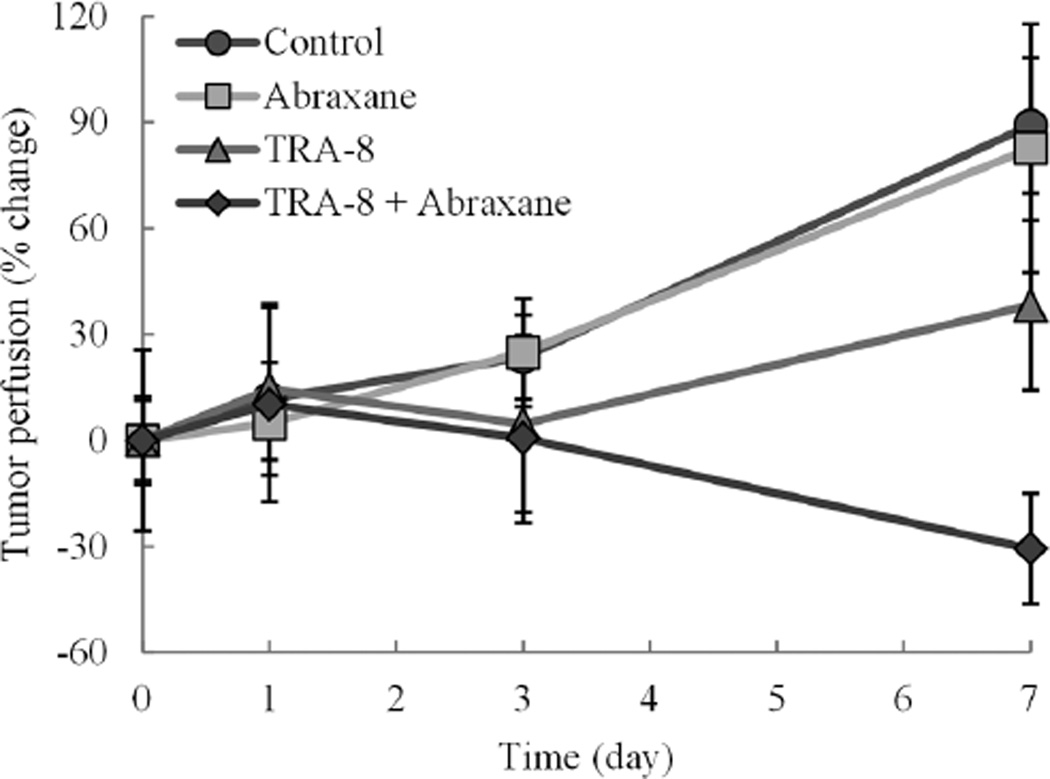
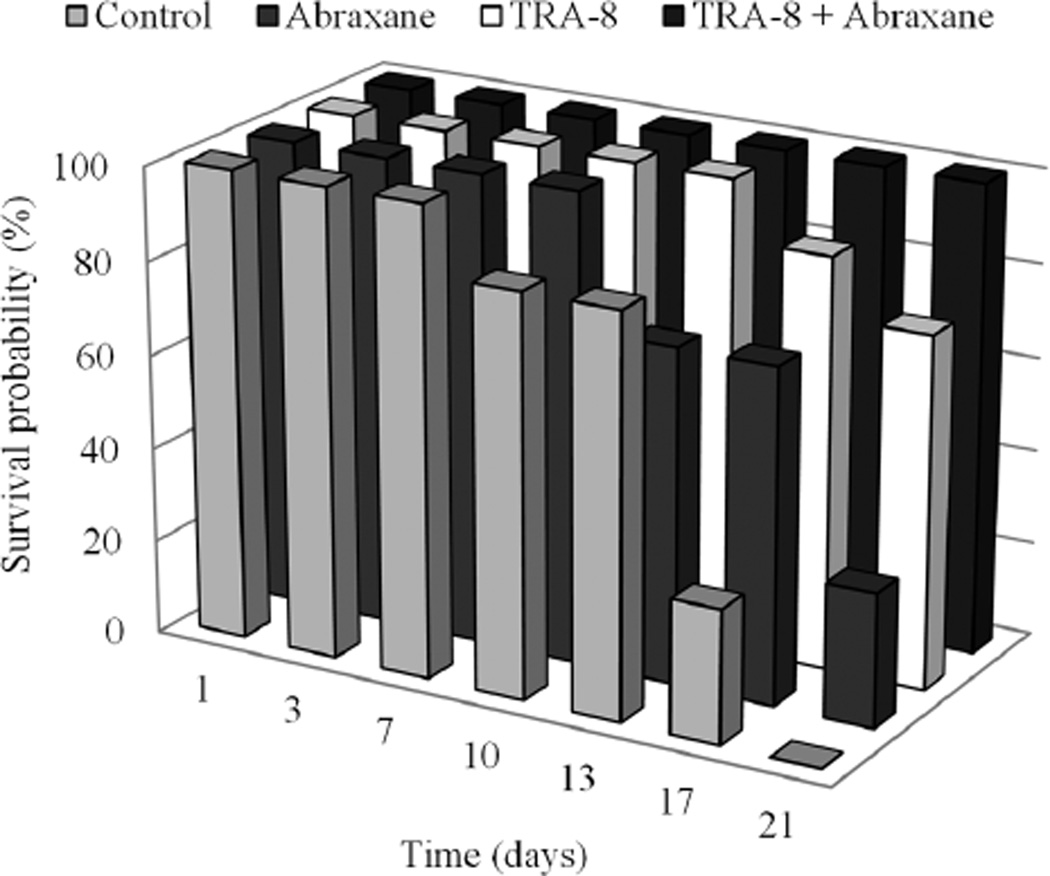
Results: Therapeutic efficacy was detected within 7 days after drug administration using parametric volumetric contrast-enhanced US imaging. Decreased tumor perfusion was observed in both the TRA-8-alone- and TRA-8 + Abraxane-dosed animals compared to control tumors (P = .17; P = .001, respectively). The reduction in perfusion observed in the TRA-8 + Abraxane group was matched with a corresponding regression in tumor size over the same period. Survival curves illustrate that the combination of TRA-8 + Abraxane improves drug efficacy compared to the same drugs administered alone. Immunohistologic analysis revealed increased levels of apoptotic activity in the TRA-8-dosed tumors, confirming enhanced antitumor effects.
Conclusions: Preliminary results are encouraging, and volumetric contrast-enhanced US-based tumor perfusion imaging may prove clinically feasible for detecting and monitoring the early antitumor effects in response to combination TRA-8 + Abraxane therapy.
Figures






Similar articles
-
Antitumor efficacy of TRA-8 anti-DR5 monoclonal antibody alone or in combination with chemotherapy and/or radiation therapy in a human breast cancer model.Clin Cancer Res. 2003 Sep 1;9(10 Pt 1):3731-41. Clin Cancer Res. 2003. PMID: 14506165
-
Effect of anti-DR5 and chemotherapy on basal-like breast cancer.Breast Cancer Res Treat. 2012 Jun;133(2):417-26. doi: 10.1007/s10549-011-1755-0. Epub 2011 Sep 7. Breast Cancer Res Treat. 2012. PMID: 21901385 Free PMC article.
-
Breast tumor xenografts: diffusion-weighted MR imaging to assess early therapy with novel apoptosis-inducing anti-DR5 antibody.Radiology. 2008 Sep;248(3):844-51. doi: 10.1148/radiol.2483071740. Radiology. 2008. PMID: 18710978 Free PMC article.
-
Combination treatment with TRA-8 anti death receptor 5 antibody and CPT-11 induces tumor regression in an orthotopic model of pancreatic cancer.Clin Cancer Res. 2007 Sep 15;13(18 Pt 2):5535s-5543s. doi: 10.1158/1078-0432.CCR-07-1075. Clin Cancer Res. 2007. PMID: 17875786 Free PMC article.
-
DCE-MRI detects early vascular response in breast tumor xenografts following anti-DR5 therapy.Mol Imaging Biol. 2011 Feb;13(1):94-103. doi: 10.1007/s11307-010-0320-2. Mol Imaging Biol. 2011. PMID: 20383593 Free PMC article.
Cited by
-
Ultrasound imaging of breast tumor perfusion and neovascular morphology.Ultrasound Med Biol. 2015 Sep;41(9):2292-302. doi: 10.1016/j.ultrasmedbio.2015.04.016. Epub 2015 Jun 24. Ultrasound Med Biol. 2015. PMID: 26116159 Free PMC article. Clinical Trial.
-
Three-dimensional evaluation of microvascular networks using contrast-enhanced ultrasound and microbubble tracking.IEEE Int Ultrason Symp. 2020 Sep;2020:10.1109/ius46767.2020.9251525. doi: 10.1109/ius46767.2020.9251525. IEEE Int Ultrason Symp. 2020. PMID: 36483236 Free PMC article.
-
Volumetric contrast-enhanced ultrasound imaging of renal perfusion.J Ultrasound Med. 2014 Aug;33(8):1427-37. doi: 10.7863/ultra.33.8.1427. J Ultrasound Med. 2014. PMID: 25063408 Free PMC article.
-
Multiscale quantification of tumor microarchitecture for predicting therapy response using dynamic contrast-enhanced ultrasound imaging.IEEE Int Ultrason Symp. 2019 Oct;2019:1173-1176. doi: 10.1109/ultsym.2019.8926152. Epub 2019 Dec 8. IEEE Int Ultrason Symp. 2019. PMID: 36518354 Free PMC article.
-
Impact of hydrostatic pressure on phase-change contrast agent activation by pulsed ultrasound.J Acoust Soc Am. 2019 Jun;145(6):3457. doi: 10.1121/1.5111345. J Acoust Soc Am. 2019. PMID: 31255129 Free PMC article.
References
-
- Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295:2492–2502. - PubMed
-
- Chaudhary PM, Eby M, Jasmin A, Bookwalter A, Murray J, Hood L. Death receptor 5, a new member of the TNFR family, and DR4 induce FADD-dependent apoptosis and activate the NF-kappaB pathway. Immunity. 1997;7:821–830. - PubMed
-
- Ashkenazi A, Dixit VM. Death receptors: signaling and modulation. Science. 1998;281:1305–1308. - PubMed
-
- Kuang AA, Diehl GE, Zhang J, Winoto A. FADD is required for DR4-and DR5-mediated apoptosis: lack of trail-induced apoptosis in FADD-deficient mouse embryonic fibroblasts. J Biol Chem. 2000;275:25065–25068. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
