

In-flight medical emergencies
- PMID: 23093989
- PMCID: PMC3461894
- DOI: 10.3238/arztebl.2012.0591
In-flight medical emergencies
Abstract
Background: One in every 10 000 to 40 000 passengers on commercial aircraft will have a medical incident while on board. Many physicians are unaware of the special features of the cabin atmosphere, the medical equipment available on airplanes, and the resulting opportunities for medical intervention.
Methods: A selective literature search was performed and supplemented with international recommendations and guidelines and with data from the Lufthansa registry.
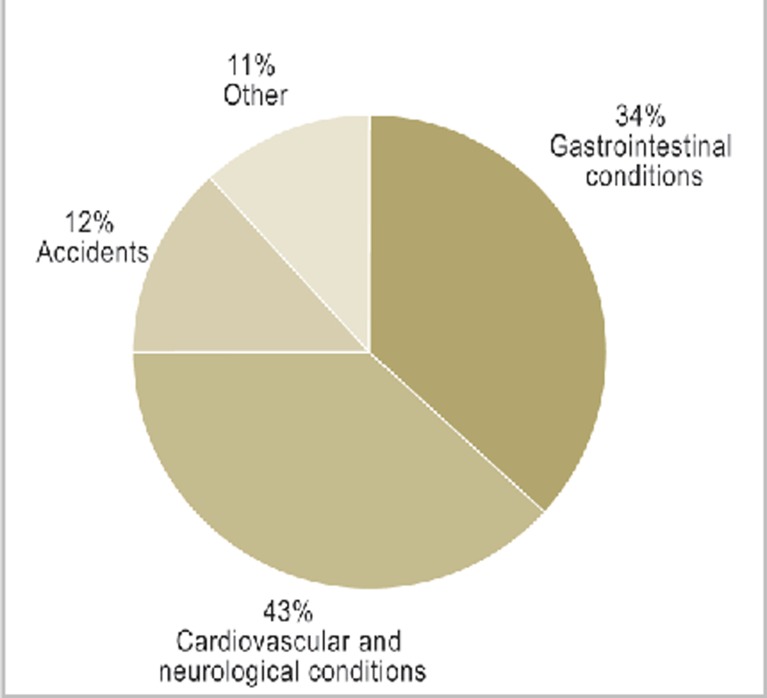
Results: Data on in-flight medical emergencies have been collected in various ways, with varying results; it is generally agreed, however, that the more common incidents include gastrointestinal conditions (diarrhea, nausea, vomiting), circulatory collapse, hypertension, stroke, and headache (including migraine). Data from the Lufthansa registry for the years 2010 and 2011 reveal the rarity of cardiopulmonary resuscitation (mean: 8 cases per year), death (12 cases per year), childbirth (1 case per year), and psychiatric incidents (81 cases per year). If one assumes that one medical incident arises for every 10 000 passengers, and that there are 400 passengers on board each flight, then one can calculate that the probability of experiencing at least one medical incident reaches 95% after 24 intercontinental flights.
Conclusion: An in-flight medical emergency is an exceptional event for the physician and all other persons involved. Physician passengers can act more effectively if they are aware of the framework conditions, the available medical equipment, and the commonly encountered medical conditions.
Figures

Comment in
-
Declaration of assumption of liability for all airlines.Dtsch Arztebl Int. 2013 Mar;110(11):191. doi: 10.3238/arztebl.2013.0191a. Epub 2013 Mar 15. Dtsch Arztebl Int. 2013. PMID: 23555323 Free PMC article. No abstract available.
-
Similar data collected.Dtsch Arztebl Int. 2013 Mar;110(11):191. doi: 10.3238/arztebl.2013.0191b. Epub 2013 Mar 15. Dtsch Arztebl Int. 2013. PMID: 23555324 Free PMC article. No abstract available.
-
Risk of VTE is small but exists.Dtsch Arztebl Int. 2013 Mar;110(11):191-2. doi: 10.3238/arztebl.2013.0191c. Epub 2013 Mar 15. Dtsch Arztebl Int. 2013. PMID: 23555325 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2013 Mar;110(11):192. doi: 10.3238/arztebl.2013.0192. Epub 2013 Mar 15. Dtsch Arztebl Int. 2013. PMID: 23555326 Free PMC article. No abstract available.
References
-
- Von Mülmann M. Die Flugzeugkabine. In: Stüben U, editor. Taschenbuch Flugmedizin. Berlin: MWV Medizinisch Wissenschaftliche Verlagsgesellschaft; 2008. pp. 3–7.
-
- Muhm JM, Rock PB, et al. Effect of aircraft-cabin altitude on passenger discomfort. N Engl J Med. 2007;357:18–27. - PubMed
-
- Wirth D, Rumberger E. Fundamentals of aviation physiology. In: Curdt-Christiansen C, Draeger J, Kriebel J, editors. Principles and practice of aviation medicine. Singapore: World Scientific Publishing; 2009. pp. 71–149.
-
- Cocks R, Liew M. Commercial aviation in-flight emergencies and the physician. Emerg Med Australas. 2007;19:1–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical