

Association of neighborhood characteristics with bystander-initiated CPR
- PMID: 23094722
- PMCID: PMC3515681
- DOI: 10.1056/NEJMoa1110700
Association of neighborhood characteristics with bystander-initiated CPR
Abstract
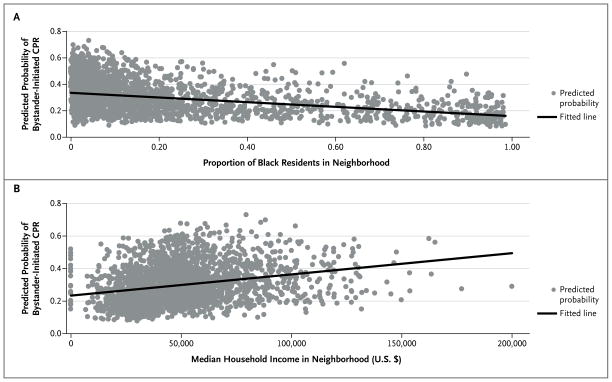
Background: For persons who have an out-of-hospital cardiac arrest, the probability of receiving bystander-initiated cardiopulmonary resuscitation (CPR) may be influenced by neighborhood characteristics.
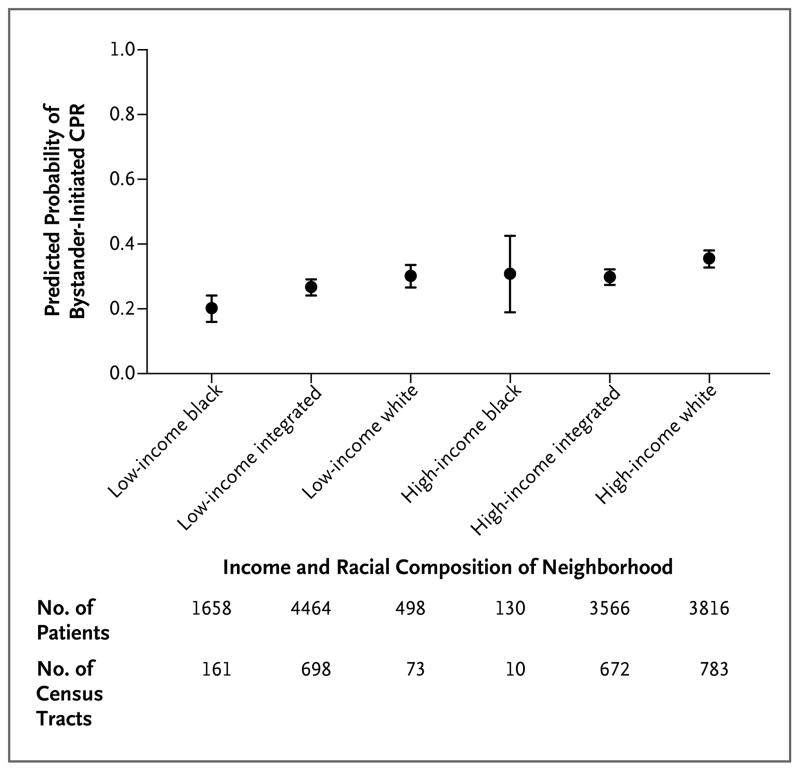
Methods: We analyzed surveillance data prospectively submitted from 29 U.S. sites to the Cardiac Arrest Registry to Enhance Survival between October 1, 2005, and December 31, 2009. The neighborhood in which each cardiac arrest occurred was determined from census-tract data. We classified neighborhoods as high-income or low-income on the basis of a median household income threshold of $40,000 and as white or black if more than 80% of the census tract was predominantly of one race. Neighborhoods without a predominant racial composition were classified as integrated. We analyzed the relationship between the median income and racial composition of a neighborhood and the performance of bystander-initiated CPR.
Results: Among 14,225 patients with cardiac arrest, bystander-initiated CPR was provided to 4068 (28.6%). As compared with patients who had a cardiac arrest in high-income white neighborhoods, those in low-income black neighborhoods were less likely to receive bystander-initiated CPR (odds ratio, 0.49; 95% confidence interval [CI], 0.41 to 0.58). The same was true of patients with cardiac arrest in neighborhoods characterized as low-income white (odds ratio, 0.65; 95% CI, 0.51 to 0.82), low-income integrated (odds ratio, 0.62; 95% CI, 0.56 to 0.70), and high-income black (odds ratio, 0.77; 95% CI, 0.68 to 0.86). The odds ratio for bystander-initiated CPR in high-income integrated neighborhoods (1.03; 95% CI, 0.64 to 1.65) was similar to that for high-income white neighborhoods.
Conclusions: In a large cohort study, we found that patients who had an out-of-hospital cardiac arrest in low-income black neighborhoods were less likely to receive bystander-initiated CPR than those in high-income white neighborhoods. (Funded by the Centers for Disease Control and Prevention and others.).
Figures
Comment in
-
Neighborhood characteristics and bystander-initiated CPR.N Engl J Med. 2013 Jan 24;368(4):391-2. doi: 10.1056/NEJMc1214188. N Engl J Med. 2013. PMID: 23343070 No abstract available.
-
Neighborhood characteristics and bystander-initiated CPR.N Engl J Med. 2013 Jan 24;368(4):391. doi: 10.1056/NEJMc1214188. N Engl J Med. 2013. PMID: 23343071 No abstract available.
References
-
- Dunne RB, Compton S, Zalenski RJ, Swor R, Welch R, Bock BF. Outcomes from out-of-hospital cardiac arrest in Detroit. Resuscitation. 2007;72:59–65. - PubMed
-
- Cummins RO. Emergency medical services and sudden cardiac arrest: the “chain of survival” concept. Annu Rev Public Health. 1993;14:313–33. - PubMed
-
- 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2005;112(24 Suppl):IV1–IV203. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials