

Tumor islands in resected early-stage lung adenocarcinomas are associated with unique clinicopathologic and molecular characteristics and worse prognosis
- PMID: 23095504
- PMCID: PMC3545070
- DOI: 10.1097/PAS.0b013e31826885fb
Tumor islands in resected early-stage lung adenocarcinomas are associated with unique clinicopathologic and molecular characteristics and worse prognosis
Abstract
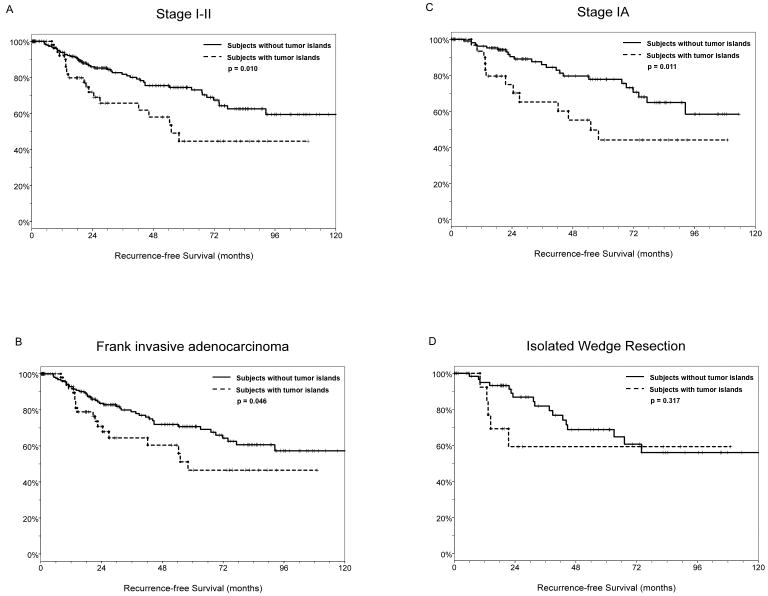
Tumor islands-large collections of tumor cells isolated within alveolar spaces-can be seen in lung adenocarcinomas. Recently we observed by 3-dimensional reconstruction that these structures were connected with each other and with the main tumor in different tissue planes, raising the possibility of tumor islands being a means of extension. However, the clinical and prognostic significance of tumor islands remains unknown. In this study, we compared clinicopathologic and molecular characteristics and prognosis of stages I to II lung adenocarcinomas with tumor islands (n=58) and those without (n=203). Lung adenocarcinomas with tumor islands were more likely to occur in smokers, exhibit higher nuclear grade and a solid or micropapillary pattern of growth, and harbor KRAS mutations. In contrast, lung adenocarcinomas without tumor islands were more likely to present as minimally invasive adenocarcinoma, show a lepidic pattern of growth, and harbor EGFR mutations. Although there was no difference in stage, the prognosis of lung adenocarcinomas with tumor islands was significantly worse than those without. The 5-year recurrence-free survival for patients with tumor islands and those without was 44.6% and 74.4%, respectively (log rank P=0.010). The survival difference remained significant (P <0.020) by multivariate analysis, and the presence of tumor islands was associated with almost 2-fold increase in the risk of recurrence. Even in the stage IA cohort, more than half of the patients with tumor islands experienced recurrence within 5 years. Thus, aggressive surveillance and/or further intervention may be indicated for patients whose tumors exhibit tumor islands.
Conflict of interest statement
For all the authors no conflicts of interest were declared.
Figures
Similar articles
-
KRAS mutations are associated with solid growth pattern and tumor-infiltrating leukocytes in lung adenocarcinoma.Mod Pathol. 2013 Oct;26(10):1307-19. doi: 10.1038/modpathol.2013.74. Epub 2013 Apr 26. Mod Pathol. 2013. PMID: 23619604 Free PMC article.
-
KRAS Mutation Is a Significant Prognostic Factor in Early-stage Lung Adenocarcinoma.Am J Surg Pathol. 2016 Dec;40(12):1579-1590. doi: 10.1097/PAS.0000000000000744. Am J Surg Pathol. 2016. PMID: 27740967 Free PMC article.
-
Differences in the survival of patients with recurrent versus de novo metastatic KRAS-mutant and EGFR-mutant lung adenocarcinomas.Cancer. 2015 Jun 15;121(12):2078-82. doi: 10.1002/cncr.29313. Epub 2015 Mar 17. Cancer. 2015. PMID: 25781862 Free PMC article.
-
High-grade lung adenocarcinomas with micropapillary and/or solid patterns: a review.Curr Opin Pulm Med. 2014 Jul;20(4):317-23. doi: 10.1097/MCP.0000000000000070. Curr Opin Pulm Med. 2014. PMID: 24852329 Review.
-
Do all lung adenocarcinomas follow a stepwise progression?Lung Cancer. 2011 Oct;74(1):7-11. doi: 10.1016/j.lungcan.2011.05.021. Epub 2011 Jun 25. Lung Cancer. 2011. PMID: 21705107 Free PMC article. Review.
Cited by
-
KRAS mutations are associated with solid growth pattern and tumor-infiltrating leukocytes in lung adenocarcinoma.Mod Pathol. 2013 Oct;26(10):1307-19. doi: 10.1038/modpathol.2013.74. Epub 2013 Apr 26. Mod Pathol. 2013. PMID: 23619604 Free PMC article.
-
Does dual-layer spectral detector CT provide added value in predicting spread through air spaces in lung adenocarcinoma? A preliminary study.Eur Radiol. 2024 Jun;34(6):4176-4186. doi: 10.1007/s00330-023-10440-6. Epub 2023 Nov 17. Eur Radiol. 2024. PMID: 37973632
-
KRAS Mutations Predict Response and Outcome in Advanced Lung Adenocarcinoma Patients Receiving First-Line Bevacizumab and Platinum-Based Chemotherapy.Cancers (Basel). 2019 Oct 9;11(10):1514. doi: 10.3390/cancers11101514. Cancers (Basel). 2019. PMID: 31600989 Free PMC article.
-
[Research Progress on Spread Through Air Spaces of Lung Cancer].Zhongguo Fei Ai Za Zhi. 2022 Jan 20;25(1):54-60. doi: 10.3779/j.issn.1009-3419.2021.101.49. Epub 2021 Dec 23. Zhongguo Fei Ai Za Zhi. 2022. PMID: 34937151 Free PMC article. Review. Chinese.
-
[Aerogenic tumor seeding : A new invasive criterion for lung carcinomas].Pathologe. 2018 May;39(3):236-241. doi: 10.1007/s00292-018-0429-7. Pathologe. 2018. PMID: 29523927 Review. German.
References
-
- Brundage MD, Davies D, Mackillop WJ. Prognostic factors in non-small cell lung cancer: A decade of progress. Chest. 2002;122:1037–1057. - PubMed
-
- Mino-Kenudson M, Mark EJ. Reflex testing for epidermal growth factor receptor mutation and anaplastic lymphoma kinase fluorescence in situ hybridization in non-small cell lung cancer. Arch Pathol Lab Med. 2011;135:655–664. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2009 (Vintage 2009 Populations) National Cancer Institute; Bethesda, MD: http://seer.cancer.gov/csr/1975_2009_pops09/
-
- Rena O, Papalia E, Ruffini E, et al. Stage i pure bronchioloalveolar carcinoma: Recurrences, survival and comparison with adenocarcinoma of the lung. Eur J Cardiothorac Surg. 2003;23:409–414. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
