

Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields
- PMID: 23095807
- PMCID: PMC3514151
- DOI: 10.1186/1477-7819-10-220
Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields
Abstract
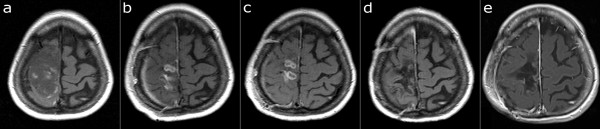
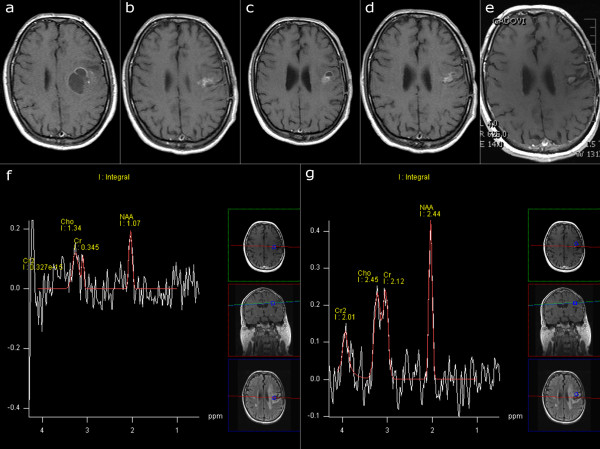
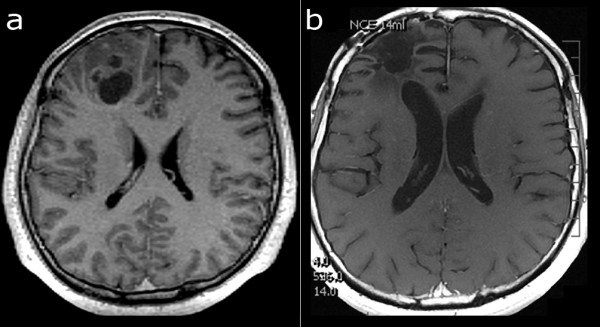
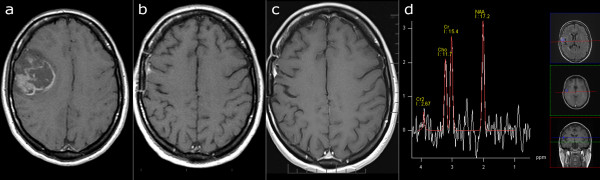
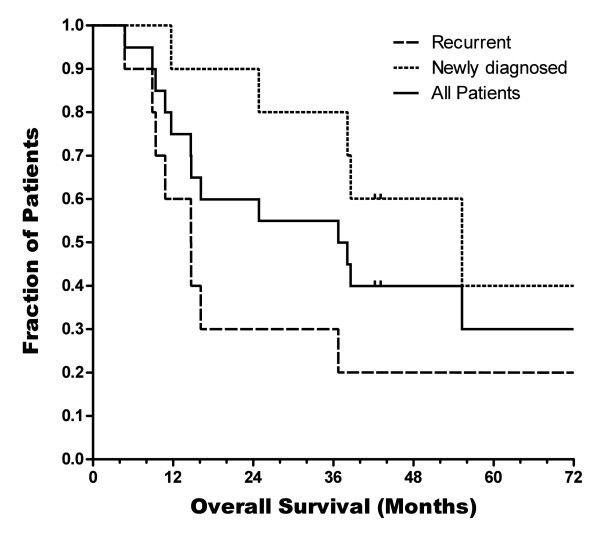
Glioblastoma multiforme (GBM) is the most common and malignant primary intracranial tumor, and has a median survival of only 10 to 14 months with only 3 to 5% of patients surviving more than three years. Recurrence (RGBM) is nearly universal, and further decreases the median survival to only five to seven months with optimal therapy. Tumor-treating fields (TTField) therapy is a novel treatment technique that has recently received CE and FDA approval for the treatment of RGBM, and is based on the principle that low intensity, intermediate frequency electric fields (100 to 300 kHz) may induce apoptosis in specific cell types. Our center was the first to apply TTField treatment to histologically proven GBM in a small pilot study of 20 individuals in 2004 and 2005, and four of those original 20 patients are still alive today. We report two cases of GBM and two cases of RGBM treated by TTField therapy, all in good health and no longer receiving any treatment more than seven years after initiating TTField therapy, with no clinical or radiological evidence of recurrence.
Figures
References
-
- Dobes M, Khurana VG, Shadbolt B, Jain S, Smith SF, Smee R, Dexter M, Cook R. Increasing incidence of glioblastoma multiforme and meningioma, and decreasing incidence of Schwannoma (2000–2008): findings of a multicenter Australian study. Surg Neurol Int. 2011;2:176. doi: 10.4103/2152-7806.90696. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
