

Multimodality image fusion to guide peripheral artery chronic total arterial occlusion recanalization in a swine carotid artery occlusion model: unblinding the interventionalist
- PMID: 23097307
- PMCID: PMC3518624
- DOI: 10.1002/ccd.24391
Multimodality image fusion to guide peripheral artery chronic total arterial occlusion recanalization in a swine carotid artery occlusion model: unblinding the interventionalist
Abstract
Objectives: To demonstrate the feasibility of magnetic resonance imaging (MRI) to X-ray fluoroscopy (XRF) image fusion to guide peripheral artery chronic total occlusion (CTO) recanalization.
Background: Endovascular peripheral artery CTO revascularization is minimally invasive, but challenging, because the occlusion is poorly visualized under XRF. Devices may steer out of the artery, which can lead to severe perforation. Merging preacquired MRI of the CTO to the live XRF display may permit upfront use of aggressive devices and improve procedural outcomes.
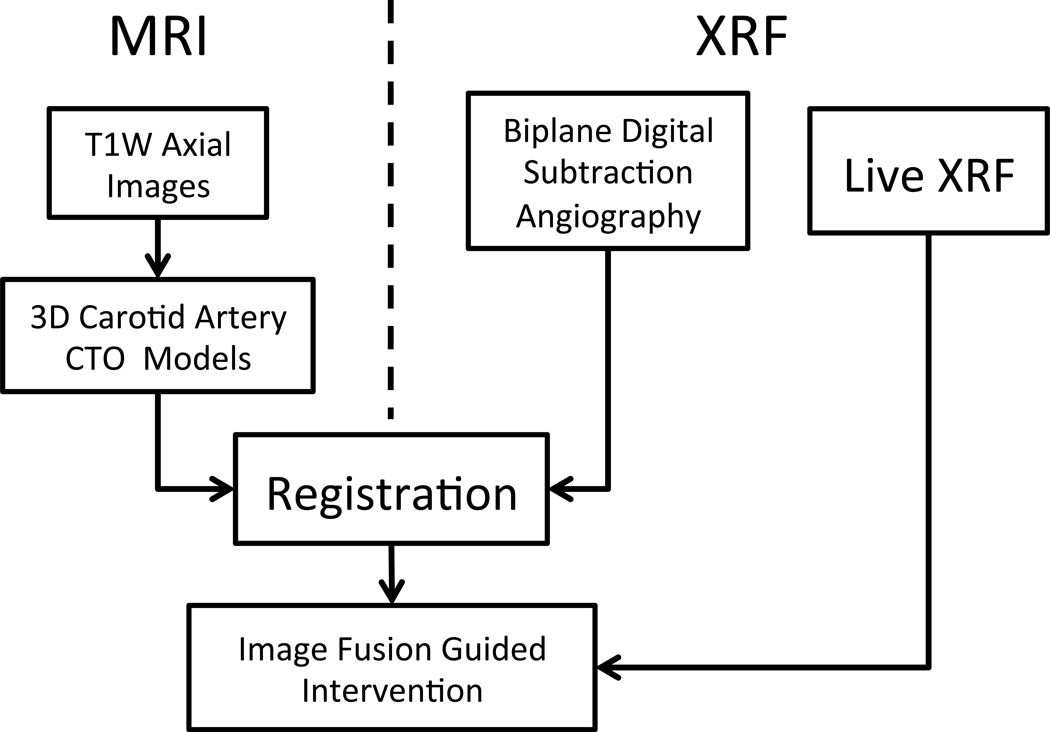
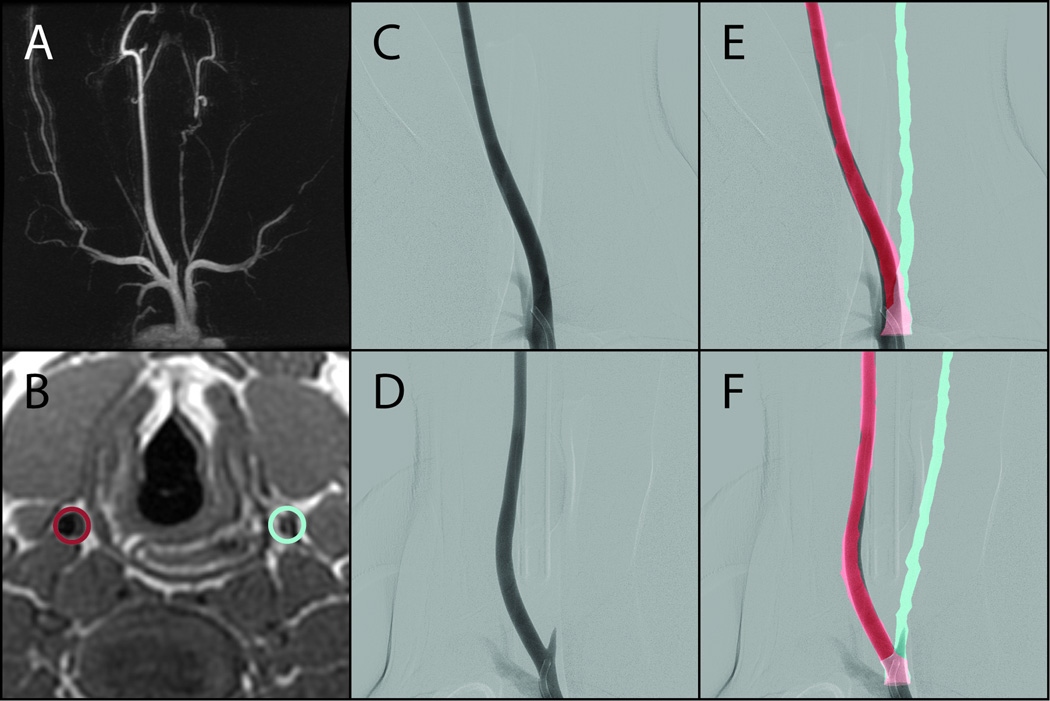
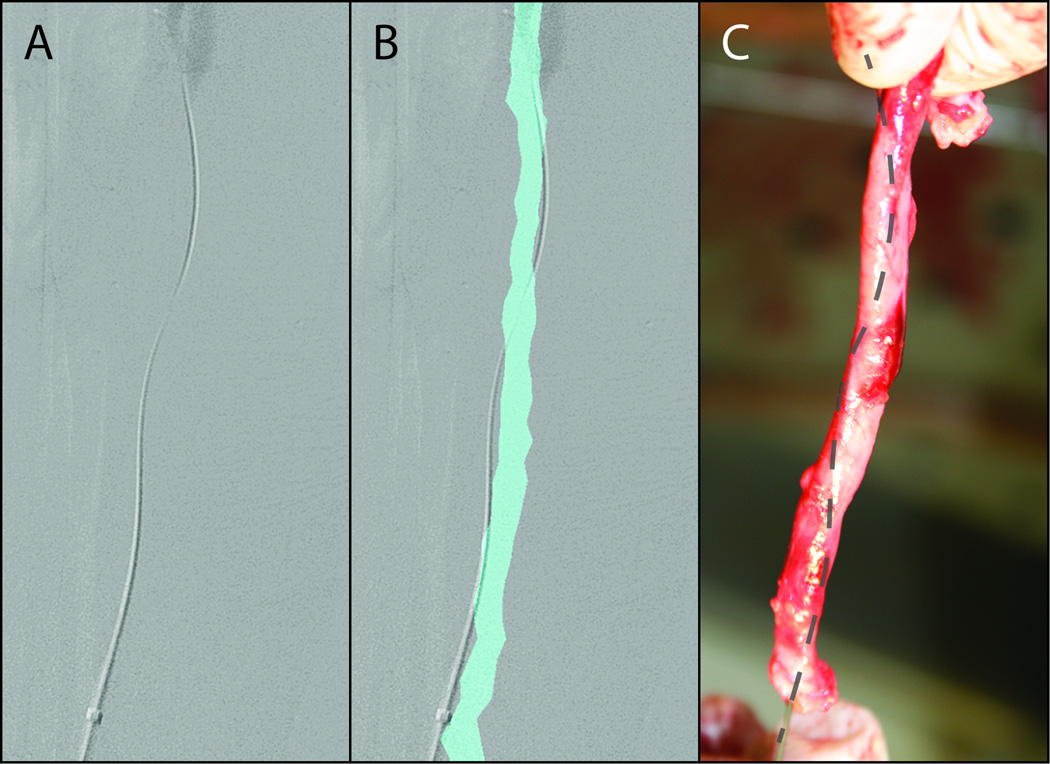
Methods: Swine carotid artery CTOs were created using a balloon injury model. Up to 8 weeks later, MRI of the carotid arteries was acquired and segmented to create three-dimensional surface models, which were then registered onto live XRF. CTO recanalization was performed using incrementally aggressive CTO devices (group A) or an upfront aggressive directed laser approach (group B). Procedural success was defined as luminal or subintimal device position without severe perforation.
Results: In this swine model, MRI to XRF fusion guidance resulted in a procedural success of 57% in group A and 100% in group B, which compared favorably to 33% using XRF alone. Fluoroscopy time was significantly less for group B (8.5 ± 2.6 min) compared to group A (48.7 ± 23.9 min), P < 0.01. Contrast dose used was similar between groups A and B.
Conclusions: MRI to XRF fusion-guided peripheral artery CTO recanalization is feasible. Multimodality image fusion may permit upfront use of aggressive CTO devices with improved procedural outcomes compared to XRF-guided procedures.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
References
-
- Diehm C, Schuster A, Allenberg JR, Darius H, Haberl R, Lange S, Pittrow D, von Stritzky B, Tepohl G, Trampisch HJ. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis. 2004;172(1):95–105. - PubMed
-
- McDermott MM, Mehta S, Greenland P. Exertional leg symptoms other than intermittent claudication are common in peripheral arterial disease. Arch Intern Med. 1999;159(4):387–392. - PubMed
-
- Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, Krook SH, Hunninghake DB, Comerota AJ, Walsh ME, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. Jama. 2001;286(11):1317–1324. - PubMed
-
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113(11):e463–e654. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, Bell K, Caporusso J, Durand-Zaleski I, Komori K, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33(Suppl 1):S1–S75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
