

Significance of deep T-wave inversions in asymptomatic athletes with normal cardiovascular examinations: practical solutions for managing the diagnostic conundrum
- PMID: 23097480
- PMCID: PMC3603779
- DOI: 10.1136/bjsports-2011-090838
Significance of deep T-wave inversions in asymptomatic athletes with normal cardiovascular examinations: practical solutions for managing the diagnostic conundrum
Abstract
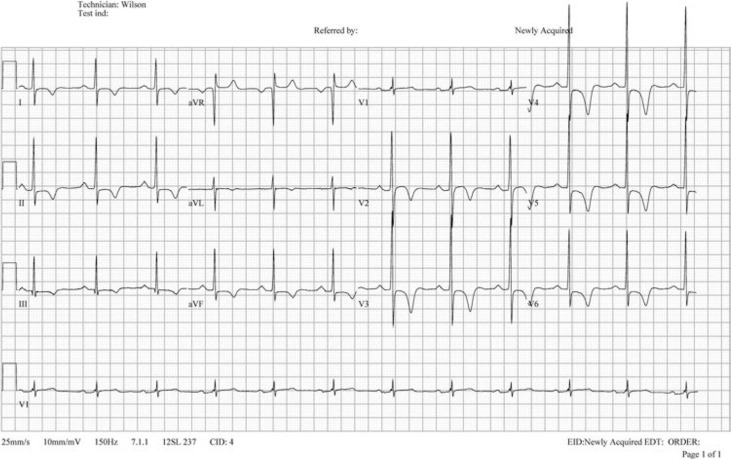
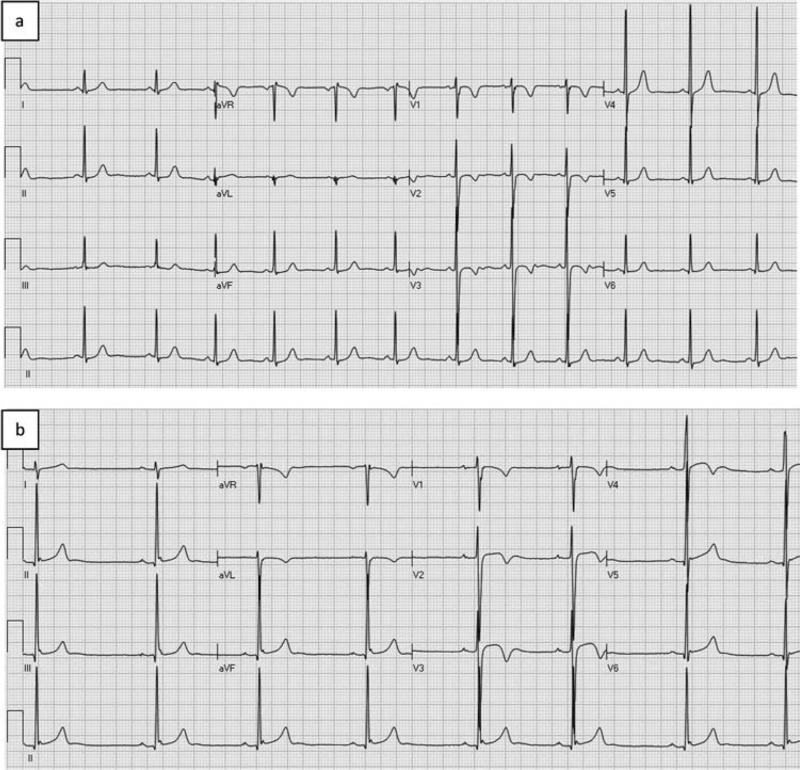
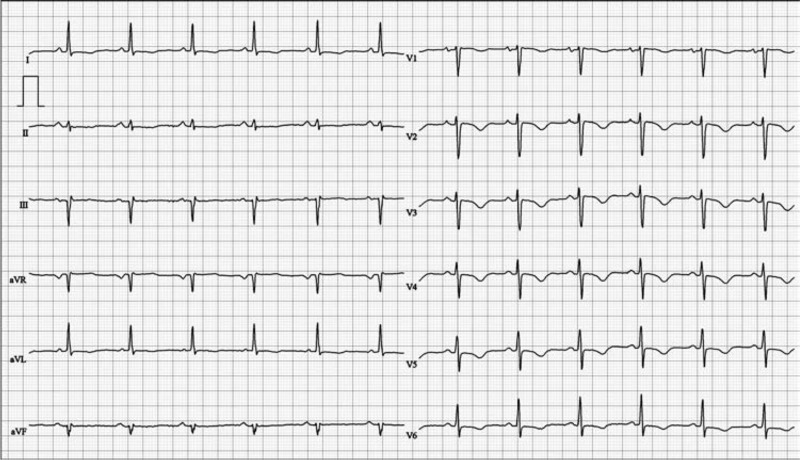
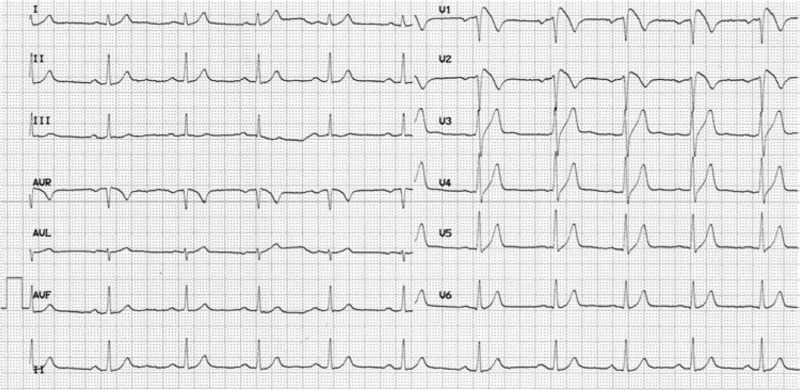
Preparticipation screening programmes for underlying cardiac pathologies are now commonplace for many international sporting organisations. However, providing medical clearance for an asymptomatic athlete without a family history of sudden cardiac death (SCD) is especially challenging when the athlete demonstrates particularly abnormal repolarisation patterns, highly suggestive of an inherited cardiomyopathy or channelopathy. Deep T-wave inversions of ≥ 2 contiguous anterior or lateral leads (but not aVR, and III) are of major concern for sports cardiologists who advise referring team physicians, as these ECG alterations are a recognised manifestation of hypertrophic cardiomyopathy (HCM) and arrhythmogenic right ventricular cardiomyopathy (ARVC). Subsequently, inverted T-waves may represent the first and only sign of an inherited heart muscle disease, in the absence of any other features and before structural changes in the heart can be detected. However, to date, there remains little evidence that deep T-wave inversions are always pathognomonic of either a cardiomyopathy or an ion channel disorder in an asymptomatic athlete following long-term follow-up. This paper aims to provide a systematic review of the prevalence of T-wave inversion in athletes and examine T-wave inversion and its relationship to structural heart disease, notably HCM and ARVC with a view to identify young athletes at risk of SCD during sport. Finally, the review proposes clinical management pathways (including genetic testing) for asymptomatic athletes demonstrating significant T-wave inversion with structurally normal hearts.
Figures

Similar articles
-
Optimal Screening Methods to Detect Cardiac Disorders in Athletes: An Evidence-Based Review.J Athl Train. 2017 Dec;52(12):1168-1170. doi: 10.4085/1062-6050-52.11.24. Epub 2017 Nov 20. J Athl Train. 2017. PMID: 29154691 Free PMC article.
-
Arrhythmogenic Right Ventricular Cardiomyopathy: Diagnosis, Risk Stratification, and Treatment.Dtsch Arztebl Int. 2025 May 2;122(9):229-234. doi: 10.3238/arztebl.m2024.0264. Dtsch Arztebl Int. 2025. PMID: 40202346 Review.
-
Outcomes of Investigating T Wave Inversion With Echocardiography in an Unselected Young Male Preparticipation Cohort.J Am Heart Assoc. 2023 Apr 4;12(7):e026975. doi: 10.1161/JAHA.122.026975. Epub 2023 Mar 21. J Am Heart Assoc. 2023. PMID: 36942750 Free PMC article.
-
Risk factors for sudden cardiac death in childhood hypertrophic cardiomyopathy: A systematic review and meta-analysis.Eur J Prev Cardiol. 2017 Jul;24(11):1220-1230. doi: 10.1177/2047487317702519. Epub 2017 May 9. Eur J Prev Cardiol. 2017. PMID: 28482693
-
Arrhythmogenic Right Ventricular Cardiomyopathy Post-Mortem Assessment: A Systematic Review.Int J Mol Sci. 2024 Feb 20;25(5):2467. doi: 10.3390/ijms25052467. Int J Mol Sci. 2024. PMID: 38473714 Free PMC article.
Cited by
-
T-wave inversions on ECG as primary manifestation of Hashimoto's disease.BMJ Case Rep. 2016 Apr 7;2016:bcr2016214949. doi: 10.1136/bcr-2016-214949. BMJ Case Rep. 2016. PMID: 27056941 Free PMC article.
-
The electrocardiographic manifestations of arrhythmogenic right ventricular dysplasia.Curr Cardiol Rev. 2014 Aug;10(3):237-45. doi: 10.2174/1573403x10666140514102928. Curr Cardiol Rev. 2014. PMID: 24827798 Free PMC article. Review.
-
Value of electro-vectorcardiogram in hypertrophic cardiomyopathy.Ann Noninvasive Electrocardiol. 2013 Jul;18(4):311-26. doi: 10.1111/anec.12067. Ann Noninvasive Electrocardiol. 2013. PMID: 23879271 Free PMC article. Review.
-
Cardiodiagnostic sex-specific differences of the female athlete in sports cardiology.Am Heart J Plus. 2022 Jun 14;17:100149. doi: 10.1016/j.ahjo.2022.100149. eCollection 2022 May. Am Heart J Plus. 2022. PMID: 38559879 Free PMC article.
-
Pattern of electrocardiographic and echocardiographic findings amongst Nigeria national football team players.Niger Med J. 2025 Jun 16;66(2):457-467. doi: 10.71480/nmj.v66i2.594. eCollection 2025 Mar-Apr. Niger Med J. 2025. PMID: 40703870 Free PMC article.
References
-
- Zeller L, Giladi H, Golan R, et al. Sudden death in a young soccer player with marked electrocardiographic repolarization abnormalities. Clin J Sport Med 2010;20:66–8 - PubMed
-
- Wilson MG, Chatard JC, Hamilton B, et al. Significance of deep T-wave inversions in an asymptomatic athlete with a family history of sudden death. Clin J Sport Med 2011;21:138–40 - PubMed
-
- Maron BJ, Ackerman MJ, Nishimura RA, et al. Task Force 4: HCM and other cardiomyopathies, mitral valve prolapse, myocarditis, and Marfan syndrome. J Am Coll Cardiol 2005;45:1340–5 - PubMed
-
- Pelliccia A, Fagard R, Bjørnstad HH, et al. Recommendations for competitive sports participation in athletes with cardiovascular disease: a consensus document from the Study Group of Sports Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2005;26:1422–45 - PubMed
-
- Sharma S. Athlete's heart–effect of age, sex, ethnicity and sporting discipline. Exp Physiol 2003;88:665–9 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources