

Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome
- PMID: 23097584
- PMCID: PMC3540040
- DOI: 10.1093/cid/cis899
Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome
Abstract
Background: Tuberculosis immune reconstitution inflammatory syndrome (IRIS) is a common cause of deterioration in human immunodeficiency virus (HIV)-infected patients receiving tuberculosis treatment after starting antiretroviral therapy (ART). Potentially life-threatening neurological involvement occurs frequently and has been suggested as a reason to defer ART.
Methods: We conducted a prospective study of HIV-infected, ART-naive patients with tuberculous meningitis (TBM). At presentation, patients started tuberculosis treatment and prednisone; ART was initiated 2 weeks later. Clinical and laboratory findings were compared between patients who developed TBM-IRIS (TBM-IRIS patients) and those who did not (non-TBM-IRIS patients). A logistic regression model was developed to predict TBM-IRIS.
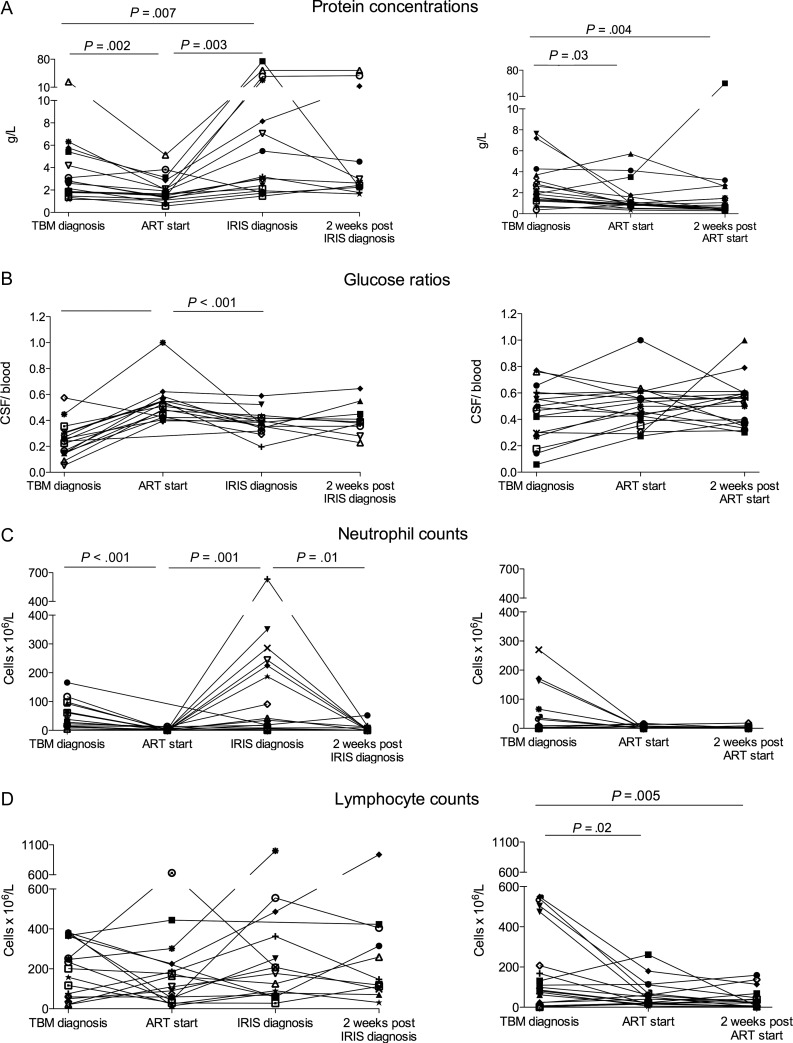
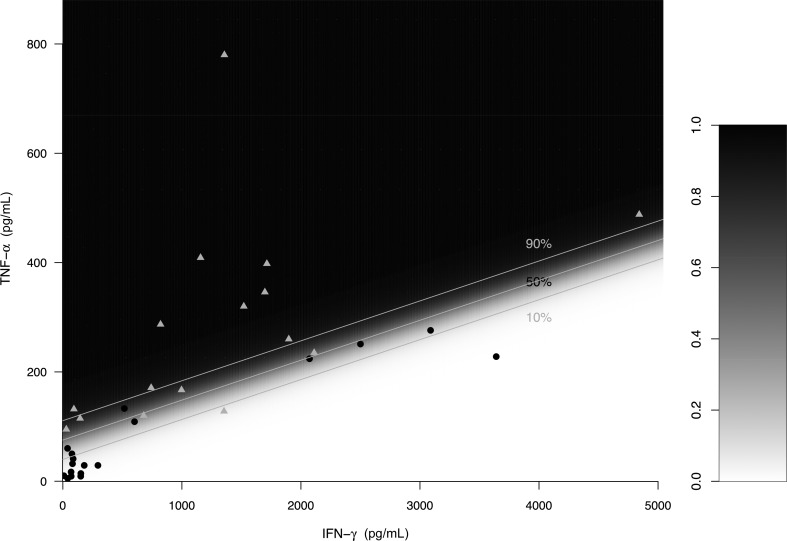
Results: Forty-seven percent (16/34) of TBM patients developed TBM-IRIS, which manifested with severe features of inflammation. At TBM diagnosis, TBM-IRIS patients had higher cerebrospinal fluid (CSF) neutrophil counts compared with non-TBM-IRIS patients (median, 50 vs 3 cells ×10(6)/L, P = .02). Mycobacterium tuberculosis was cultured from CSF of 15 TBM-IRIS patients (94%) compared with 6 non-TBM-IRIS patients (33%) at time of TBM diagnosis; relative risk of developing TBM-IRIS if CSF was Mycobacterium tuberculosis culture positive = 9.3 (95% confidence interval [CI], 1.4-62.2). The combination of high CSF tumor necrosis factor (TNF)-α and low interferon (IFN)-γ at TBM diagnosis predicted TBM-IRIS (area under the curve = 0.91 [95% CI, .53-.99]).
Conclusions: TBM-IRIS is a frequent, severe complication of ART in HIV-associated TBM and is characterized by high CSF neutrophil counts and Mycobacterium tuberculosis culture positivity at TBM presentation. The combination of CSF IFN-γ and TNF-α concentrations may predict TBM-IRIS and thereby be a means to individualize patients to early or deferred ART.
Figures

References
-
- Meintjes G, Rabie H, Wilkinson RJ, Cotton MF. Tuberculosis-associated immune reconstitution inflammatory syndrome and unmasking of tuberculosis by antiretroviral therapy. Clin Chest Med. 2009;30:797–810. - PubMed
