

Respiratory Consequences of Mild-to-Moderate Obesity: Impact on Exercise Performance in Health and in Chronic Obstructive Pulmonary Disease
- PMID: 23097698
- PMCID: PMC3477561
- DOI: 10.1155/2012/818925
Respiratory Consequences of Mild-to-Moderate Obesity: Impact on Exercise Performance in Health and in Chronic Obstructive Pulmonary Disease
Abstract
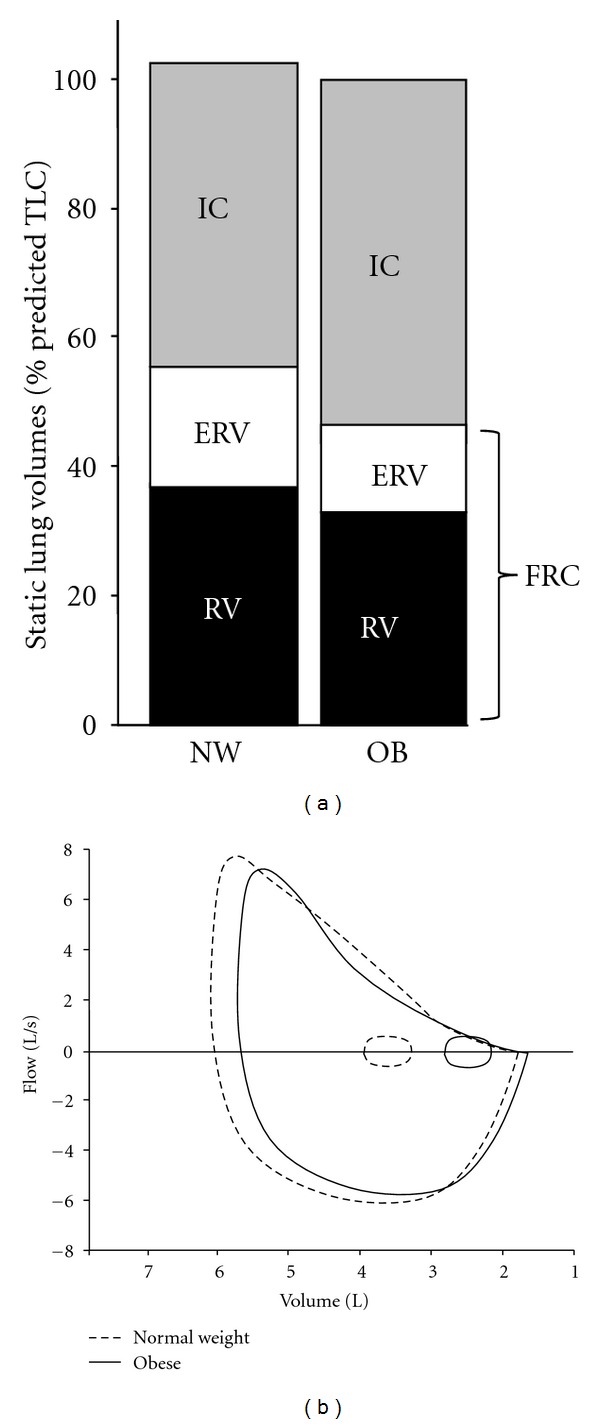
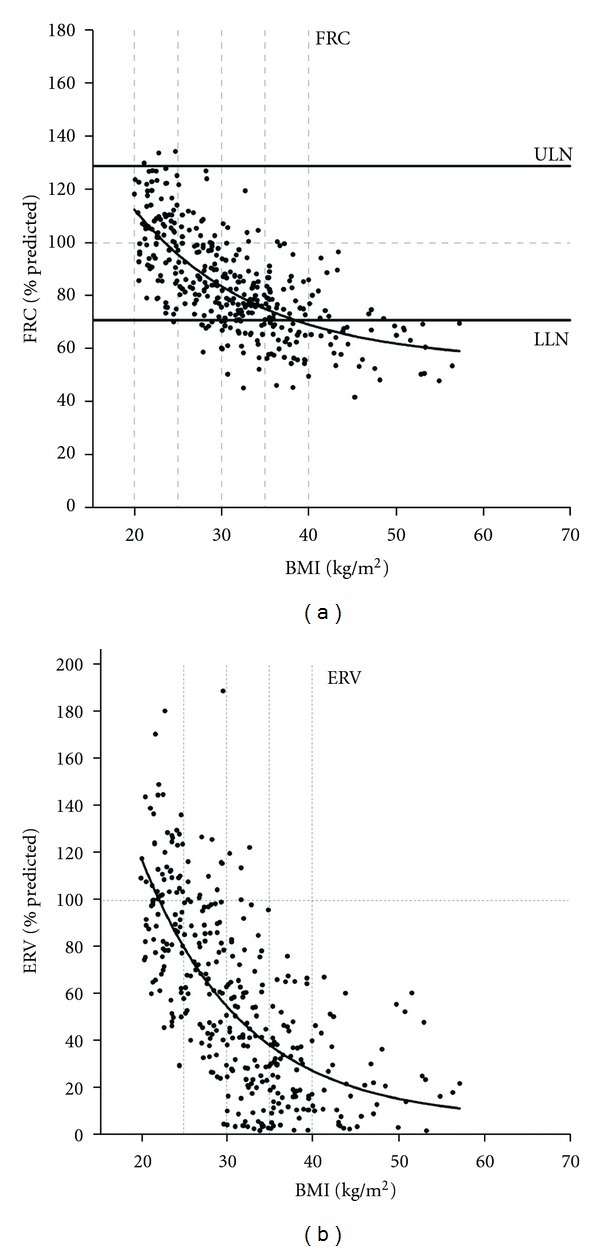
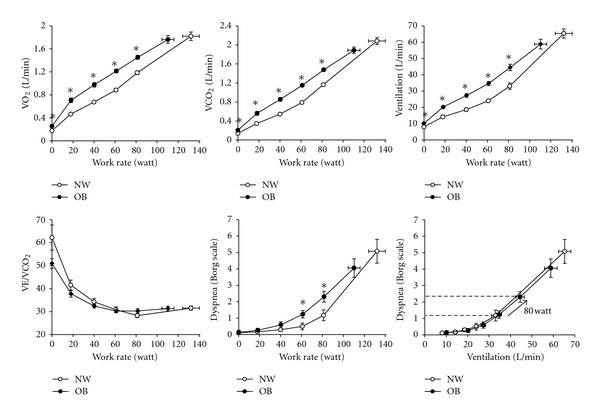
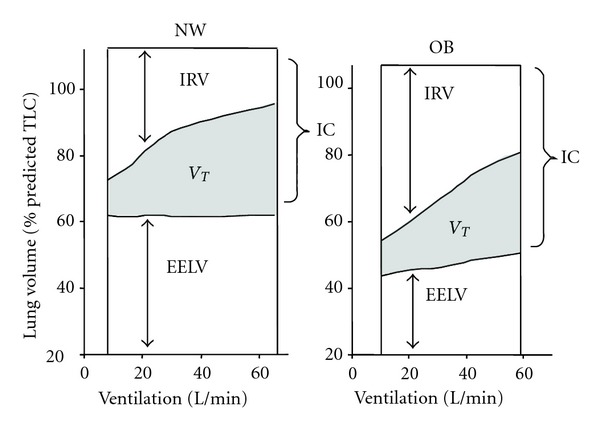
In many parts of the world, the prevalence of obesity is increasing at an alarming rate. The association between obesity, multiple comorbidities, and increased mortality is now firmly established in many epidemiological studies. However, the link between obesity and exercise intolerance is less well studied and is the focus of this paper. Although exercise limitation is likely to be multifactorial in obesity, it is widely believed that the respiratory mechanical constraints and the attendant dyspnea are important contributors. In this paper, we examined the evidence that critical ventilatory constraint is a proximate source of exercise limitation in individuals with mild-to-moderate obesity. We first reviewed existing information on exercise performance, including ventilatory and perceptual response patterns, in obese individuals who are otherwise healthy. We then considered the impact of obesity in patients with preexisting respiratory mechanical abnormalities due to chronic obstructive pulmonary disease (COPD), with particular reference to the effect on dyspnea and exercise performance. Our main conclusion, based on the existing and rather sparse literature on the subject, is that abnormalities of dynamic respiratory mechanics are not likely to be the dominant source of dyspnea and exercise intolerance in otherwise healthy individuals or in patients with COPD with mild-to-moderate obesity.
Figures
References
-
- Wang YC, McPherson K, Marsh T, et al. Health and economic burden of the projected obesity trends in the USA and the UK. The Lancet. 2011;378:815–825. - PubMed
-
- Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. Journal of the American Medical Association. 2003;289(2):187–193. - PubMed
-
- Martínez-González MÁ, Martínez JA, Hu FB, Gibney MJ, Kearney J. Physical inactivity, sedentary lifestyle and obesity in the European Union. International Journal of Obesity. 1999;23(11):1192–1201. - PubMed
LinkOut - more resources
Full Text Sources
