

FGF23 is correlated with iron status but not with inflammation and decreases after iron supplementation: a supplementation study
- PMID: 23098062
- PMCID: PMC3523041
- DOI: 10.1186/1687-9856-2012-27
FGF23 is correlated with iron status but not with inflammation and decreases after iron supplementation: a supplementation study
Abstract
Background: Recent studies have described relationships between iron status and fibroblast growth factor-23 (FGF23) but the possible confounding effects of inflammation on iron status have not been considered. The aims of this study were a) to consider a relationship between FGF23 and inflammation b) to identify relationships between iron status and FGF23 whilst correcting for inflammation and c) to assess the relationship between changes in FGF23 and iron status after supplementation.
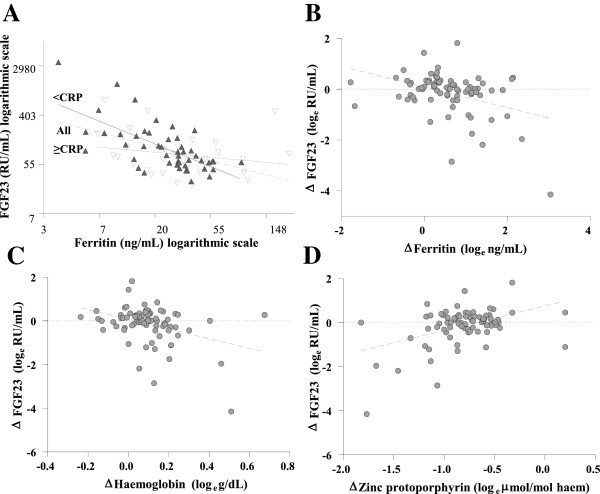
Study design and methodology: Blood samples from an iron supplementation study in children (n=79) were collected at baseline and after 3 months supplementation with iron sulphate. The children were from a rural Gambian population where rates of iron deficiency and infection/inflammation are high. This study identified cross-sectional and longitudinal relationships between FGF23, inflammation (C-reactive protein (CRP)) and iron status (ferritin, haemoglobin, and zinc protoporphyrin). CRP ≥ 5 mg/dL was used to indicate inflammation and FGF23 ≥ 125 RU/mL was considered elevated.
Results: FGF23 was not significantly correlated with CRP. At baseline, all markers of iron status were significantly correlated with FGF23. Ferritin was the strongest independent inverse predictor of FGF23 in subjects with and without elevated CRP (coefficient (SE)): All subjects=-0.57 (0.12), R2=22.3%, P≤0.0001; subjects with CRP < 5 mg/dL=-0.89 (0.14), R2=38.9%, P≤0.0001. FGF23 was elevated in 28% of children at baseline and 16% post supplementation (P=0.1). Improved iron status was associated with a decrease in FGF23 concentration in univariate (ferritin =-0.41 (0.11), R2=14.1%, P=0.0004; haemoglobin=-2.22 (0.64), R2=12.5%, P=0.0008; zinc protoporphyrin=1.12 (0.26), R2=18.6%, P≤0.0001) and multivariate analysis (R2=33.1%; ferritin=-0.36 (0.10), P=0.0007, haemoglobin = -1.83 (0.61), P=0.004, zinc protoporphyrin=0.62 (0.26), P=0.02).
Conclusions: Iron status rather than inflammation is a negative predictor of plasma FGF23 concentration. Improvements in iron status following iron supplementation are associated with a significant decrease in FGF23 concentration.
Figures
References
-
- Farrow EG, Yu X, Summers LJ, Davis SI, Fleet JC, Allen MR, Robling AG, Stayrook KR, Jideonwo V, Magers MJ, Garringer HJ, Vidal R, Chan RJ, Goodwin CB, Hui SL, Peacock M, White KE. Iron deficiency drives an autosomal dominant hypophosphatemic rickets (adhr) phenotype in fibroblast growth factor-23 (FGF23) knock-in mice. Proc Natl Acad Sci USA. 2011;108:E1146–E1155. doi: 10.1073/pnas.1110905108. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
