

External validation of the Bayesian Estimated Tools for Survival (BETS) models in patients with surgically treated skeletal metastases
- PMID: 23098538
- PMCID: PMC3556063
- DOI: 10.1186/1471-2407-12-493
External validation of the Bayesian Estimated Tools for Survival (BETS) models in patients with surgically treated skeletal metastases
Abstract
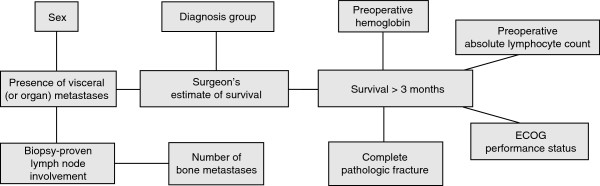
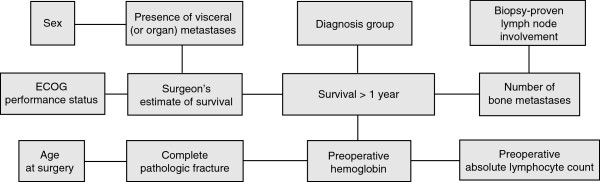
Background: We recently developed two Bayesian networks, referred to as the Bayesian-Estimated Tools for Survival (BETS) models, capable of estimating the likelihood of survival at 3 and 12 months following surgery for patients with operable skeletal metastases (BETS-3 and BETS-12, respectively). In this study, we attempted to externally validate the BETS-3 and BETS-12 models using an independent, international dataset.
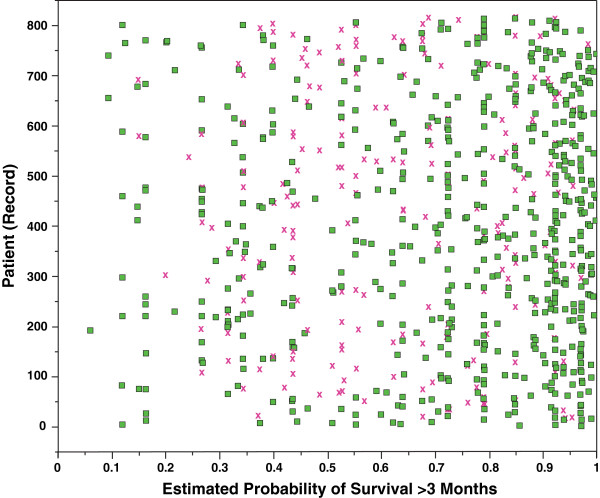
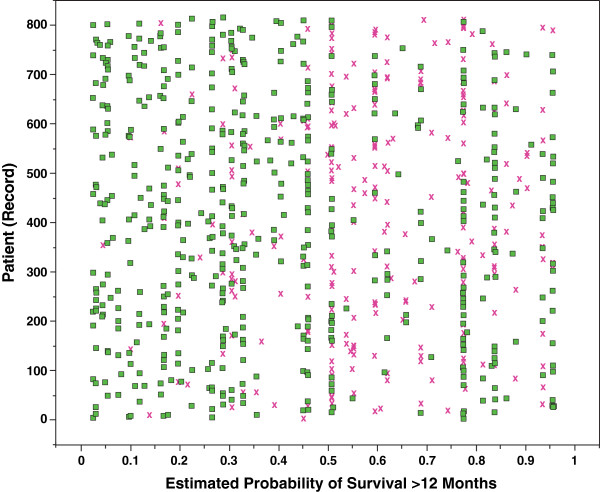
Methods: Data were collected from the Scandinavian Skeletal Metastasis Registry for patients with extremity skeletal metastases surgically treated at eight major Scandinavian referral centers between 1999 and 2009. These data were applied to the BETS-3 and BETS-12 models, which generated a probability of survival at 3 and 12 months for each patient. Model robustness was assessed using the area under the receiver-operating characteristic curve (AUC). An analysis of incorrect estimations was also performed.
Results: Our dataset contained 815 records with adequate follow-up information to establish survival at 12 months. All records were missing data including the surgeon's estimate of survival, which was previously shown to be a first-degree associate of survival in both models. The AUCs for the BETS-3 and BETS-12 models were 0.79 and 0.76, respectively. Incorrect estimations by both models were more commonly optimistic than pessimistic.
Conclusions: The BETS-3 and BETS-12 models were successfully validated using an independent dataset containing missing data. These models are the first validated tools for accurately estimating postoperative survival in patients with operable skeletal metastases of the extremities and can provide the surgeon with valuable information to support clinical decisions in this patient population.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
