

Imatinib mesylate for plexiform neurofibromas in patients with neurofibromatosis type 1: a phase 2 trial
- PMID: 23099009
- PMCID: PMC5380388
- DOI: 10.1016/S1470-2045(12)70414-X
Imatinib mesylate for plexiform neurofibromas in patients with neurofibromatosis type 1: a phase 2 trial
Abstract
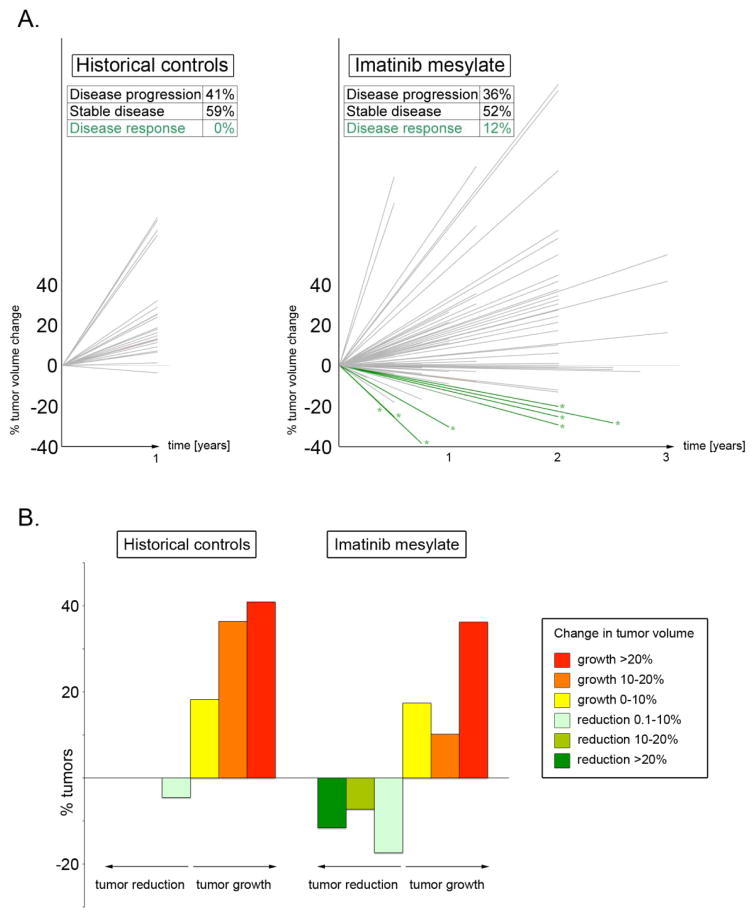
Background: Plexiform neurofibromas are slow-growing chemoradiotherapy-resistant tumours arising in patients with neurofibromatosis type 1 (NF1). Currently, there are no viable therapeutic options for patients with plexiform neurofibromas that cannot be surgically removed because of their proximity to vital body structures. We undertook an open-label phase 2 trial to test whether treatment with imatinib mesylate can decrease the volume burden of clinically significant plexiform neurofibromas in patients with NF1.
Methods: Eligible patients had to be aged 3-65 years, and to have NF1 and a clinically significant plexiform neurofibroma. Patients were treated with daily oral imatinib mesylate at 220 mg/m(2) twice a day for children and 400 mg twice a day for adults for 6 months. The primary endpoint was a 20% or more reduction in plexiform size by sequential volumetric MRI imaging. Clinical data were analysed on an intention-to-treat basis; a secondary analysis was also done for those patients able to take imatinib mesylate for 6 months. This trial is registered with ClinicalTrials.gov, number NCT01673009.
Findings: Six of 36 patients (17%, 95% CI 6-33), enrolled on an intention-to-treat basis, had an objective response to imatinib mesylate, with a 20% or more decrease in tumour volume. Of the 23 patients who received imatinib mesylate for at least 6 months, six (26%, 95% CI 10-48) had a 20% or more decrease in volume of one or more plexiform tumours. The most common adverse events were skin rash (five patients) and oedema with weight gain (six). More serious adverse events included reversible grade 3 neutropenia (two), grade 4 hyperglycaemia (one), and grade 4 increases in aminotransferase concentrations (one).
Interpretation: Imatinib mesylate could be used to treat plexiform neurofibromas in patients with NF1. A multi-institutional clinical trial is warranted to confirm these results.
Funding: Novartis Pharmaceuticals, the Indiana University Simon Cancer Centre, and the Indiana University Herman B Wells Center for Pediatric Research.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST
The authors have no financial or personal interests that would inappropriately influence their work on this manuscript.
Figures

Comment in
-
Treatment for plexiform neurofibromas in patients with NF1.Lancet Oncol. 2012 Dec;13(12):1175-6. doi: 10.1016/S1470-2045(12)70435-7. Epub 2012 Oct 23. Lancet Oncol. 2012. PMID: 23099008 No abstract available.
Similar articles
-
Treatment for plexiform neurofibromas in patients with NF1.Lancet Oncol. 2012 Dec;13(12):1175-6. doi: 10.1016/S1470-2045(12)70435-7. Epub 2012 Oct 23. Lancet Oncol. 2012. PMID: 23099008 No abstract available.
-
Marrow signal changes observed in follow-up whole-body MRI studies in children and young adults with neurofibromatosis type 1 treated with imatinib mesylate (Gleevec) for plexiform neurofibromas.Pediatr Radiol. 2012 Oct;42(10):1218-22. doi: 10.1007/s00247-012-2440-0. Epub 2012 Jun 22. Pediatr Radiol. 2012. PMID: 22722872 Clinical Trial.
-
Imatinib mesylate (Glivec) inhibits Schwann cell viability and reduces the size of human plexiform neurofibroma in a xenograft model.J Neurooncol. 2010 May;98(1):11-9. doi: 10.1007/s11060-009-0049-4. Epub 2009 Nov 17. J Neurooncol. 2010. PMID: 19921098
-
Pathogenesis of plexiform neurofibroma: tumor-stromal/hematopoietic interactions in tumor progression.Annu Rev Pathol. 2012;7:469-95. doi: 10.1146/annurev-pathol-011811-132441. Epub 2011 Nov 7. Annu Rev Pathol. 2012. PMID: 22077553 Free PMC article. Review.
-
Selumetinib for children with neurofibromatosis type 1 and plexiform neurofibromas that can't be removed by surgery, and impact on how the condition affects caregivers: a plain language summary.J Comp Eff Res. 2025 Mar;14(3):e240184. doi: 10.57264/cer-2024-0184. Epub 2025 Jan 21. J Comp Eff Res. 2025. PMID: 39835668 Free PMC article. Review.
Cited by
-
Treatment of neurofibromatosis type 1.Curr Treat Options Neurol. 2015 Jun;17(6):355. doi: 10.1007/s11940-015-0355-4. Curr Treat Options Neurol. 2015. PMID: 25917340
-
Preclinical assessment of the anticancer drug response of plexiform neurofibroma tissue using primary cultures.J Clin Neurol. 2015 Apr;11(2):172-7. doi: 10.3988/jcn.2015.11.2.172. J Clin Neurol. 2015. PMID: 25851896 Free PMC article.
-
The new deal: a potential role for secreted vesicles in innate immunity and tumor progression.Front Immunol. 2015 Feb 24;6:66. doi: 10.3389/fimmu.2015.00066. eCollection 2015. Front Immunol. 2015. PMID: 25759690 Free PMC article. Review.
-
After Nf1 loss in Schwann cells, inflammation drives neurofibroma formation.Neurooncol Adv. 2019 Nov 22;2(Suppl 1):i23-i32. doi: 10.1093/noajnl/vdz045. eCollection 2020 Jul. Neurooncol Adv. 2019. PMID: 32642730 Free PMC article. Review.
-
Image segmentation of plexiform neurofibromas from a deep neural network using multiple b-value diffusion data.Sci Rep. 2020 Oct 20;10(1):17857. doi: 10.1038/s41598-020-74920-1. Sci Rep. 2020. PMID: 33082502 Free PMC article.
References
-
- Williams VC, Lucas J, Babcock MA, Gutmann DH, Korf B, Maria BL. Neurofibromatosis type 1 revisited. Pediatrics. 2009;123:124–33. - PubMed
-
- Wolkenstein P, Rodriguez D, Ferkal S, et al. Impact of neurofibromatosis 1 upon quality of life in childhood: a cross-sectional study of 79 cases. Br J Dermatol. 2009;160:844–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
