

Socioeconomic inequalities in risk factors for non communicable diseases in low-income and middle-income countries: results from the World Health Survey
- PMID: 23102008
- PMCID: PMC3507902
- DOI: 10.1186/1471-2458-12-912
Socioeconomic inequalities in risk factors for non communicable diseases in low-income and middle-income countries: results from the World Health Survey
Abstract
Background: Monitoring inequalities in non communicable disease risk factor prevalence can help to inform and target effective interventions. The prevalence of current daily smoking, low fruit and vegetable consumption, physical inactivity, and heavy episodic alcohol drinking were quantified and compared across wealth and education levels in low- and middle-income country groups.
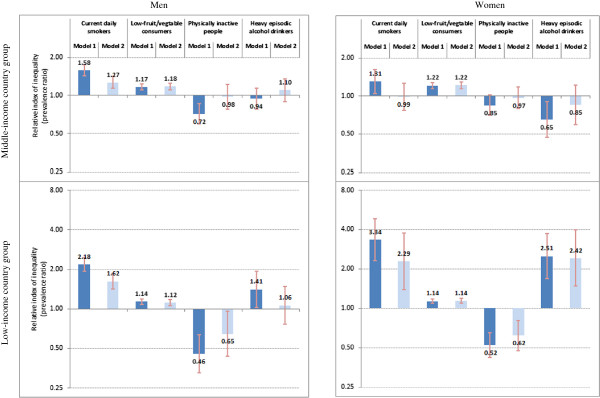
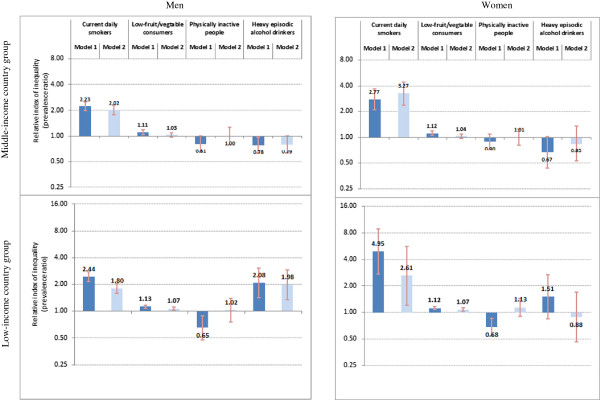
Methods: This study included self-reported data from 232,056 adult participants in 48 countries, derived from the 2002-2004 World Health Survey. Data were stratified by sex and low- or middle-income country status. The main outcome measurements were risk factor prevalence rates reported by wealth quintile and five levels of educational attainment. Socioeconomic inequalities were measured using the slope index of inequality, reflecting differences in prevalence rates, and the relative index of inequality, reflecting the prevalence ratio between the two extremes of wealth or education accounting for the entire distribution. Data were adjusted for confounding factors: sex, age, marital status, area of residence, and country of residence.
Results: Smoking and low fruit and vegetable consumption were significantly higher among lower socioeconomic groups. The highest wealth-related absolute inequality was seen in smoking among men of low- income country group (slope index of inequality 23.0 percentage points; 95% confidence interval 19.6, 26.4). The slope index of inequality for low fruit and vegetable consumption across the entire distribution of education was around 8 percentage points in both sexes and both country income groups. Physical inactivity was less prevalent in populations of low socioeconomic status, especially in low-income countries (relative index of inequality: (men) 0.46, 95% confidence interval 0.33, 0.64; (women) 0.52, 95% confidence interval 0.42, 0.65). Mixed patterns were found for heavy drinking.
Conclusions: Disaggregated analysis of the prevalence of non-communicable disease risk factors demonstrated different patterns and varying degrees of socioeconomic inequalities across low- and middle-income settings. Interventions should aim to reach and achieve sustained benefits for high-risk populations.
Figures
References
-
- World Health Organization. Global status report on noncommunicable diseases. World Health Organization, Geneva; 2011.
-
- World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. World Health Organization, Geneva; 2009.
-
- World Health Organization. 2008–2013 action plan for the global strategy for the prevention and control of noncommunicable diseases: prevent and control cardiovascular diseases, cancers, chronic respiratory diseases and diabetes. World Health Organization, Geneva; 2008.
-
- World Health Organization. Preventing chronic diseases: a vital investment: WHO global report. World Health Organization, Geneva; 2005.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
