

Continuous renal replacement therapy for children ≤10 kg: a report from the prospective pediatric continuous renal replacement therapy registry
- PMID: 23102589
- PMCID: PMC5545826
- DOI: 10.1016/j.jpeds.2012.08.044
Continuous renal replacement therapy for children ≤10 kg: a report from the prospective pediatric continuous renal replacement therapy registry
Abstract
Objective: To report circuit characteristics and survival analysis in children weighing ≤10 kg enrolled in the Prospective Pediatric Continuous Renal Replacement Therapy (ppCRRT) Registry.
Study design: We conducted prospective cohort analysis of the ppCRRT Registry to: (1) evaluate survival differences in children ≤10 kg compared with other children; (2) determine demographic and clinical differences between surviving and non-surviving children ≤10 kg; and (3) describe continuous renal replacement therapy (CRRT) circuit characteristics differences in children ≤5 kg versus 5-10 kg.
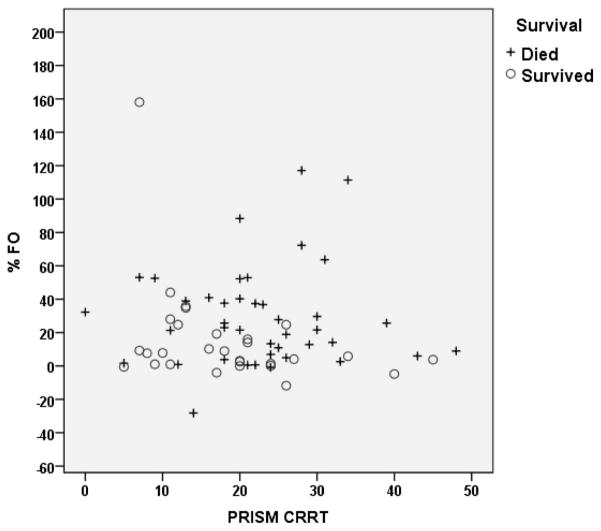
Results: The ppCRRT enrolled 84 children ≤10 kg between January 2001 and August 2005 from 13 US tertiary centers. Children ≤10 kg had lower survival rates than children >10 kg (36/84 [43%] versus 166/260 [64%]; P < .001). In children ≤10 kg, survivors were more likely to have fewer days in intensive care unit prior to CRRT, lower Pediatric Risk of Mortality 2 scores at intensive care unit admission and lower mean airway pressure (P(aw)), higher urine output, and lower percent fluid overload (FO) at CRRT initiation. Adjusted regression analysis revealed that Pediatric Risk of Mortality 2 scores, FO, and decreased urine output were associated with mortality. Compared with circuits from children 5-10 kg at CRRT initiation, circuits from children ≤5 kg more commonly used blood priming for initiation, heparin anticoagulation, and higher blood flows/effluent flows for body weight.
Conclusion: Mortality is more common in children who are ≤10 kg at the time of CRRT initiation. Like other CRRT populations, urine output and FO at CRRT initiation are independently associated with mortality. CRRT prescription differs in small children.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures

References
-
- Warady BA, Bunchman T. Dialysis therapy for children with acute renal failure: survey results. Pediatr Nephrol. 2000;15:11–3. - PubMed
-
- Symons JM, Brophy PD, Gregory MJ, McAfee N, Somers MJ, Bunchman TE, et al. Continuous renal replacement therapy in children up to 10 kg. Am J Kidney Dis. 2003;41:984–9. - PubMed
-
- Sutherland SM, Zappitelli M, Alexander SR, Chua AN, Brophy PD, Bunchman TE, et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis. 2010;55:316–25. - PubMed
-
- Flores FX, Brophy PD, Symons JM, Fortenberry JD, Chua AN, Alexander SR, et al. Continuous renal replacement therapy (CRRT) after stem cell transplantation. A report from the prospective pediatric CRRT Registry Group. Pediatr Nephrol. 2008;23:625–30. - PubMed
-
- Hackbarth R, Bunchman TE, Chua AN, Somers MJ, Baum M, Symons JM, et al. The effect of vascular access location and size on circuit survival in pediatric continuous renal replacement therapy: a report from the ppCRRT Registry. Int J Artif Organs. 2007;30:1116–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
