

Prophylactic stabilization for bone metastases, myeloma, or lymphoma: do we need to protect the entire bone?
- PMID: 23104043
- PMCID: PMC3563787
- DOI: 10.1007/s11999-012-2656-1
Prophylactic stabilization for bone metastases, myeloma, or lymphoma: do we need to protect the entire bone?
Abstract
Background: The current operative standard of care for disseminated malignant bone disease suggests stabilizing the entire bone to avoid the need for subsequent operative intervention but risks of doing so include complications related to embolic phenomena.
Questions/purposes: We questioned whether progression and reoperation occur with enough frequency to justify additional risks of longer intramedullary devices.
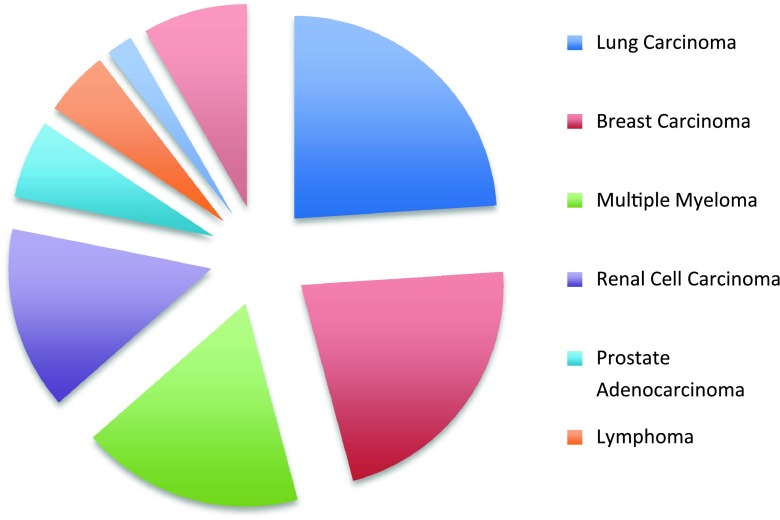
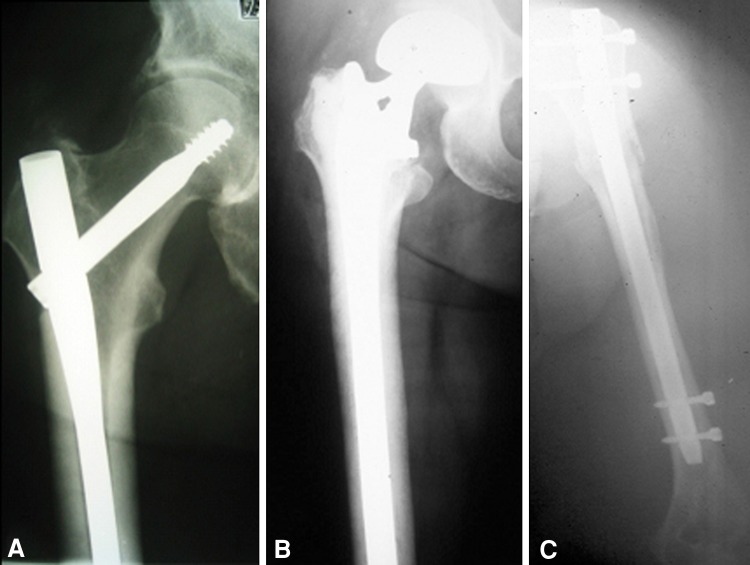
Methods: A retrospective chart review was done for 96 patients with metastases, myeloma, or lymphoma who had undergone stabilization or arthroplasty of impending or actual femoral or humeral pathologic fractures using an approach favoring intramedullary fixation devices and long-stem arthroplasty. Incidence of progressive bone disease, reoperation, and complications associated with fixation and arthroplasty devices in instrumented femurs or humeri was determined.
Results: At minimum 0 months followup (mean, 11 months; range, 0-72 months), 80% of patients had died. Eleven of 96 patients (12%) experienced local bony disease progression; eight had local progression at the original site, two had progression at originally recognized discretely separate lesions, and one had a new lesion develop in the bone that originally was surgically treated. Six subjects (6.3%) required repeat operative intervention for symptomatic failure. Twelve (12.5%) patients experienced physiologic nonfatal complications potentially attributable to embolic phenomena from long intramedullary implants.
Conclusions: Because most patients in this series were treated with the intent to protect the bone with long intramedullary implants when possible, the reoperation rate may be lower than if the entire bone had not been protected. However, the low incidence of disease progression apart from originally identified lesions (one of 96) was considerably lower than the physiologic complication rate (12 of 96) potentially attributable to long intramedullary implants.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures

Comment in
-
Editor's Spotlight/Take 5: Prophylactic stabilization for bone metastases, myeloma, or lymphoma: do we need to protect the entire bone? (DOI 10.1007/s11999-012-2656-1).Clin Orthop Relat Res. 2013 Mar;471(3):703-5. doi: 10.1007/s11999-012-2714-8. Clin Orthop Relat Res. 2013. PMID: 23208121 Free PMC article. No abstract available.
-
Letter to the editor: Prophylactic stabilization for bone metastases, myeloma, or lymphoma: do we need to protect the entire bone?Clin Orthop Relat Res. 2013 Jul;471(7):2407. doi: 10.1007/s11999-013-2994-7. Epub 2013 Apr 18. Clin Orthop Relat Res. 2013. PMID: 23595512 Free PMC article. No abstract available.
References
-
- Ampil FL, Sadasivan KK. Prophylactic and therapeutic fixation of weight-bearing long bones with metastatic cancer. South Med J. 2001;94:394–396. - PubMed
-
- Berman AT, Hermantin FU, Horowitz SM. Metastatic disease of the hip: evaluation and treatment. J Am Acad Orthop Surg. 1997;5:79–86. - PubMed
-
- Damron TA. Metastatic disease. In: Damron TA, editor. Orthopaedic Essentials: Oncology and Basic Science. Baltimore, MD, USA: Lippincott Williams & Wilkins; 2007.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
