

Manualized therapy for PTSD: flexing the structure of cognitive processing therapy
- PMID: 23106761
- PMCID: PMC3538790
- DOI: 10.1037/a0030600
Manualized therapy for PTSD: flexing the structure of cognitive processing therapy
Abstract
Objective: This study tested a modified cognitive processing therapy (MCPT) intervention designed as a more flexible administration of the protocol. Number of sessions was determined by client progress toward a priori defined end-state criteria, "stressor sessions" were inserted when necessary, and therapy was conducted by novice CPT clinicians.
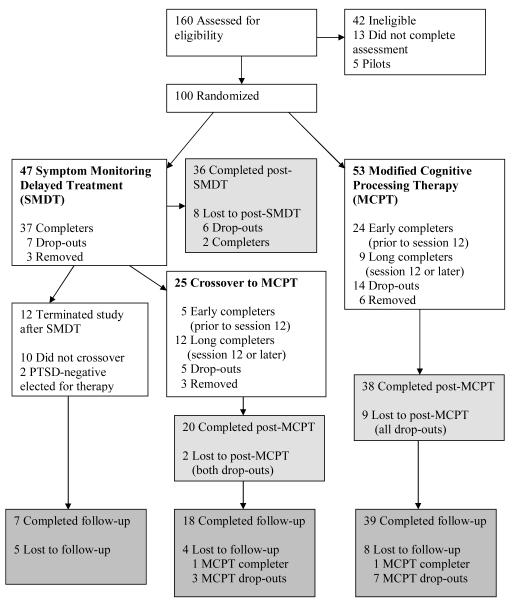
Method: A randomized, controlled, repeated measures, semicrossover design was utilized (a) to test the relative efficacy of the MCPT intervention compared with a symptom-monitoring delayed treatment (SMDT) condition and (b) to assess within-group variation in change with a sample of 100 male and female interpersonal trauma survivors with posttraumatic stress disorder (PTSD).
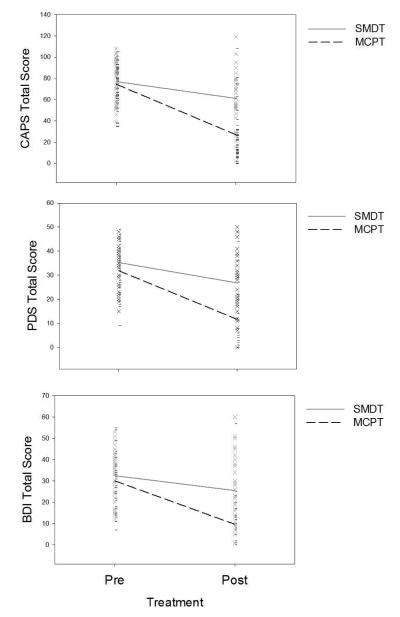
Results: Hierarchical linear modeling analyses revealed that MCPT evidenced greater improvement on all primary (PTSD and depression) and secondary (guilt, quality of life, general mental health, social functioning, and health perceptions) outcomes compared with SMDT. After the conclusion of SMDT, participants crossed over to MCPT, resulting in a combined MCPT sample (n = 69). Of the 50 participants who completed MCPT, 58% reached end-state criteria prior to the 12th session, 8% at Session 12, and 34% between Sessions 12 and 18. Maintenance of treatment gains was found at the 3-month follow-up, with only 2 of the treated sample meeting criteria for PTSD. Use of stressor sessions did not result in poorer treatment outcomes.
Conclusions: Findings suggest that individuals respond at a variable rate to CPT, with significant benefit from additional therapy when indicated and excellent maintenance of gains. Insertion of stressor sessions did not alter the efficacy of the therapy.
Figures
References
-
- American Psychological Association . Diagnostic and statistical manual of mental disorders. 4th ed., text revision Author; Washington DC: 2000.
-
- Barlow DH. The effectiveness of psychotherapy: Science and policy. Clinical Psychology: Science and Practice. 1996;3:236–240. doi:10.1111/j.1468-2850.1996.tb00075.x.
-
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory. 2nd ed The Psychological Corporation; San Antonio, TX: 1996.
-
- Bjornsson AJ. Beyond the “psychological placebo”: Specifying the nonspecific in psychotherapy. Clinical Psychology Science and Practice. 2011;18:113–118.
