

Amyloid deposition, hypometabolism, and longitudinal cognitive decline
- PMID: 23109153
- PMCID: PMC3786871
- DOI: 10.1002/ana.23650
Amyloid deposition, hypometabolism, and longitudinal cognitive decline
Abstract
Objective: Using data from the Alzheimer's Disease Neuroimaging Initiative (ADNI) population, we examined (1) cross-sectional relationships between amyloid deposition, hypometabolism, and cognition, and (2) associations between amyloid and hypometabolism measurements and longitudinal cognitive measurements.
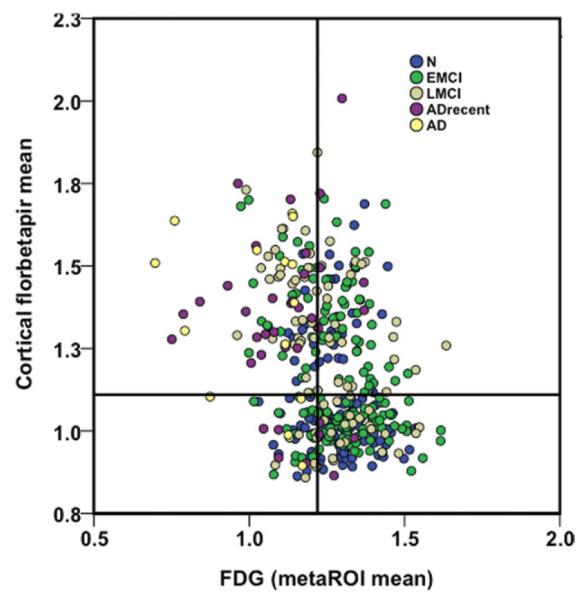
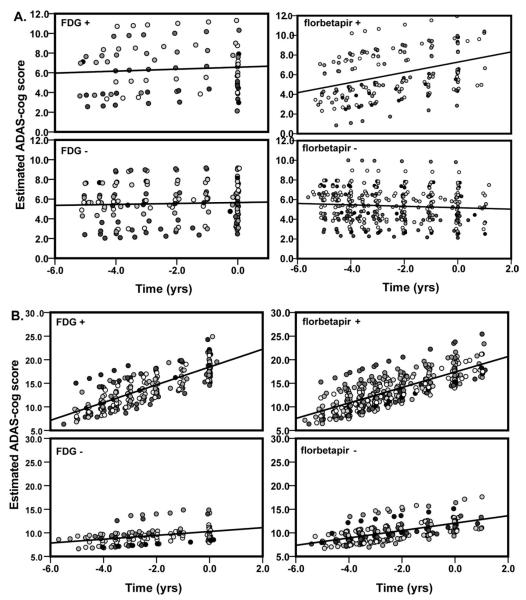
Methods: We examined associations between mean cortical florbetapir uptake, mean (18) F-fluorodeoxyglucose-positron emission tomography (FDG-PET) within a set of predefined regions, and Alzhiemer's Disease Assessment Scale (ADAS-cog) performance in 426 ADNI participants (126 normal, 162 early mild cognitive impairment [EMCI], 85 late MCI [LMCI], 53 Alzheimer disease [AD] patients). For a subset of these (76 normal, 81 LMCI) we determined whether florbetapir and FDG-PET were associated with retrospective decline in longitudinal ADAS-cog measurements.
Results: Twenty-nine percent of normal subjects, 43% of EMCI patients, 62% of LMCI patients, and 77% of AD patients were categorized as florbetapir positive. Florbetapir was negatively associated with concurrent FDG and ADAS-cog in both MCI groups. In longitudinal analyses, florbetapir-positive subjects in both normal and LMCI groups had greater ongoing ADAS-cog decline than those who were florbetapir negative. However, in normal subjects, florbetapir positivity was associated with greater ADAS-cog decline than FDG, whereas in LMCI, FDG positivity was associated with greater decline than florbetapir.
Interpretation: Although both hypometabolism and β-amyloid (Aβ) deposition are detectable in normal subjects and all diagnostic groups, Aβ showed greater associations with cognitive decline in normal participants. In view of the minimal cognitive deterioration overall in this group, this suggests that amyloid deposition has an early and subclinical impact on cognition that precedes metabolic changes. At moderate and later stages of disease (LMCI/AD), hypometabolism becomes more pronounced and more closely linked to ongoing cognitive decline.
Copyright © 2012 American Neurological Association.
Figures

References
-
- Drzezga A, Lautenschlager N, Siebner H, et al. Cerebral metabolic changes accompanying conversion of mild cognitive impairment into Alzheimer’s disease: a PET follow-up study. Eur J Nucl Med Mol Imaging. 2003;30:1104–1113. - PubMed
